Uro-Oncology focuses on the diagnosis and treatment of cancers affecting the urinary tract and the male reproductive organs, including the kidney, bladder, prostate, and testicles.
With advanced technology and minimally invasive techniques, Dr. Rohit Kaushal provides comprehensive care — from early detection to surgical management — ensuring effective treatment with faster recovery and improved quality of life for patients.
Prostate cancer is one of the most common cancers among men. When detected early, while still confined to the prostate gland, it is referred to as localized prostate cancer. At this stage, various effective treatment options are available, offering excellent chances for successful outcomes.
Localized prostate cancer means the cancer cells are found only within the prostate gland and have not spread to other parts of the body. Early detection, often through PSA screening and biopsy, is crucial for identifying localized disease and enabling timely intervention.
Choosing the right treatment for localized prostate cancer depends on several factors, including the cancer’s aggressiveness (Gleason score), PSA levels, tumor stage, the patient’s age, overall health, and personal preferences. Common treatment approaches include:
Active Surveillance: For very low-risk cancers, some patients may opt for active surveillance. This involves closely monitoring the cancer with regular PSA tests, prostate exams, and sometimes repeat biopsies, delaying treatment unless there are signs of progression. This approach helps avoid immediate treatment side effects while ensuring the cancer is managed.
Radical Prostatectomy: This is a surgical procedure to remove the entire prostate gland and sometimes surrounding lymph nodes.
Open Radical Prostatectomy: Involves a single incision to remove the prostate.
Laparoscopic Radical Prostatectomy: A minimally invasive approach using several small incisions and specialized instruments.
Robotic-Assisted Radical Prostatectomy: Utilizes a robotic system to enhance the surgeon’s precision and visualization, often leading to less blood loss, reduced pain, and faster recovery.
Radiation Therapy: This treatment uses high-energy rays to kill cancer cells or prevent them from growing.
External Beam Radiation Therapy (EBRT): Radiation is delivered from a machine outside the body.
Brachytherapy: Radioactive seeds are placed directly into the prostate gland, delivering a high dose of radiation to the cancer while sparing surrounding tissues.
Hormone Therapy: While primarily used for advanced prostate cancer, it can sometimes be used in conjunction with radiation therapy for higher-risk localized disease to shrink the tumor.
Navigating the options for localized prostate cancer can be complex. It is essential to have an open discussion with a multidisciplinary team, including urologists, radiation oncologists, and medical oncologists, to understand the potential benefits, risks, and side effects associated with each treatment.
Factors to consider when making your decision include:
The specific characteristics of your cancer
Your overall health and existing medical conditions
Potential impact on urinary, bowel, and sexual function
Your lifestyle and personal preferences
Localized prostate cancer is highly treatable, and advancements in medical science continue to improve outcomes and minimize treatment-related side effects. A personalized approach, guided by expert medical advice, is key to selecting the most appropriate treatment plan and achieving the best possible quality of life. Regular follow-up and monitoring are crucial after any treatment to ensure long-term success.
Locally advanced prostate cancer refers to a stage where the cancer has spread beyond the prostate gland but has not yet metastasized to distant parts of the body. This diagnosis requires a comprehensive and often multidisciplinary approach to treatment, focusing on controlling the disease and improving patient outcomes.
In locally advanced prostate cancer, cancer cells have extended through the prostate capsule into surrounding tissues, such as the seminal vesicles or nearby lymph nodes. While not yet metastatic, it carries a higher risk of recurrence and progression compared to localized disease.
Accurate staging through advanced imaging (MRI, CT, PET scans) and biopsy is crucial to determine the extent of the disease and guide treatment decisions.
Given the complexity of locally advanced prostate cancer, treatment often involves a combination of modalities tailored to the individual patient’s health, cancer characteristics (e.g., Gleason score, PSA levels), and personal preferences.
Common treatment approaches include:
Radical Prostatectomy:
Description: Surgical removal of the entire prostate gland, along with seminal vesicles and sometimes nearby lymph nodes.
Approach: Can be performed as open surgery, laparoscopic surgery, or with robotic assistance. Robotic prostatectomy offers enhanced precision, visualization, and often quicker recovery for suitable candidates.
Goal: To remove all cancerous tissue and achieve clear surgical margins.
Radiation Therapy:
Description: Uses high-energy rays to kill cancer cells.
Types:
External Beam Radiation Therapy (EBRT): Delivered from a machine outside the body. Advanced techniques like Intensity-Modulated Radiation Therapy (IMRT) and Stereotactic Body Radiation Therapy (SBRT) allow for precise targeting, minimizing damage to surrounding healthy tissues.
Brachytherapy: Involves placing radioactive seeds directly into the prostate gland.
Goal: To destroy cancer cells and control local disease progression. Often combined with hormone therapy for enhanced effectiveness.
Hormone Therapy (Androgen Deprivation Therapy – ADT):
Description: Prostate cancer growth is often fueled by male hormones (androgens). Hormone therapy aims to reduce the levels of these hormones or block their action.
Methods: Medications can be used to stop testosterone production (e.g., LHRH agonists/antagonists) or block testosterone’s effect on prostate cancer cells (e.g., anti-androgens).
Goal: To shrink the tumor, slow its growth, and make radiation therapy more effective. It is frequently used in conjunction with radiation therapy or after prostatectomy for high-risk cases.
Active Surveillance:
Description: For select patients with low-risk features of locally advanced prostate cancer who may prefer to delay definitive treatment, active surveillance involves close monitoring of the cancer with regular PSA tests, DREs, and repeat biopsies.
Considerations: This approach is less common for locally advanced disease but may be discussed in specific, carefully evaluated circumstances.
Effective management of locally advanced prostate cancer typically involves a multidisciplinary team, including urologists, radiation oncologists, medical oncologists, and pathologists. This collaborative approach ensures that each patient receives a personalized treatment plan that considers all aspects of their disease and overall health.
Locally advanced prostate cancer requires a robust and individualized treatment strategy to optimize outcomes. With advancements in surgical techniques, radiation delivery, and systemic therapies, patients have access to highly effective options designed to control the disease, manage symptoms, and preserve quality of life. Consulting with a specialist to discuss the most appropriate treatment path is crucial for individuals diagnosed with this condition.
Prostate cancer is a prevalent malignancy among men, and while often curable in its early stages, it can sometimes progress to an advanced form known as metastatic prostate cancer. This occurs when cancer cells spread from the prostate gland to other parts of the body, most commonly the bones, lymph nodes, liver, or lungs.
When prostate cancer metastasizes, it means the disease has spread beyond the local confines of the prostate. This advanced stage requires a different approach to treatment, focusing on managing the widespread disease, alleviating symptoms, and improving quality of life. Unlike localized prostate cancer, metastatic disease is generally not curable, but it is treatable, with significant advancements in recent years offering effective management strategies.
Prostate cancer cells can spread through:
The Lymphatic System: Cancer cells can enter the lymphatic vessels and travel to nearby or distant lymph nodes.
The Bloodstream: Cancer cells can enter blood vessels and travel to distant organs, where they can form new tumors.
Diagnosis typically involves a combination of:
PSA (Prostate-Specific Antigen) Blood Test: Elevated and rising PSA levels can indicate advanced disease.
Imaging Studies: Scans such as bone scans, CT scans, and MRI scans are used to identify the location and extent of metastases.
Biopsy: While not always necessary for diagnosis of metastasis if primary cancer is confirmed, sometimes biopsies of suspicious metastatic sites may be performed.
The goal of treatment for metastatic prostate cancer is to control the cancer’s growth, manage symptoms, and maintain the patient’s quality of life. Treatment strategies are often systemic, addressing cancer cells throughout the body, and may include:
Androgen Deprivation Therapy (ADT): This is the cornerstone of treatment. Since prostate cancer often relies on male hormones (androgens like testosterone) to grow, ADT aims to reduce androgen levels or block their action. This can be achieved through:
LHRH Agonists/Antagonists: Medications that stop the testicles from producing testosterone.
Anti-androgens: Medications that block testosterone from binding to cancer cells.
Bilateral Orchiectomy: Surgical removal of the testicles, which also stops testosterone production.
New Generation Androgen Receptor-Targeting Agents: These oral medications (e.g., abiraterone, enzalutamide, apalutamide, darolutamide) further block androgen production or receptor signaling, often used in combination with or after ADT.
Chemotherapy: Used for hormone-resistant metastatic prostate cancer, or when the disease is aggressive, to kill cancer cells throughout the body.
Radiation Therapy: Can be used to target specific metastatic sites, particularly in bones, to alleviate pain and prevent fractures.
Bone-Targeted Therapies: Medications (e.g., denosumab, zoledronic acid) are used to strengthen bones and prevent skeletal-related events in patients with bone metastases.
Immunotherapy: A newer treatment approach that uses the body’s immune system to fight cancer cells, currently used for specific subtypes of prostate cancer (e.g., those with DNA repair gene mutations).
Precision Medicine/Targeted Therapy: For patients with specific genetic mutations in their tumors, targeted drugs (e.g., PARP inhibitors) may be an option.
Living with metastatic prostate cancer involves managing the disease itself and the side effects of its treatments. A multidisciplinary team, including urologists, oncologists, pain management specialists, and supportive care professionals, works to:
Control Pain: Especially from bone metastases, through medication, radiation, or other interventions.
Manage Treatment Side Effects: Such as fatigue, hot flashes, bone thinning, and sexual dysfunction.
Provide Emotional and Psychological Support: Addressing the mental health challenges that can accompany a cancer diagnosis.
Metastatic prostate cancer is a serious diagnosis, but significant advancements in treatment options have transformed its management. While typically not curable, a personalized, comprehensive treatment plan can effectively control the disease, manage symptoms, and significantly enhance a patient’s quality of life. Continuous research promises even more innovative solutions in the future.
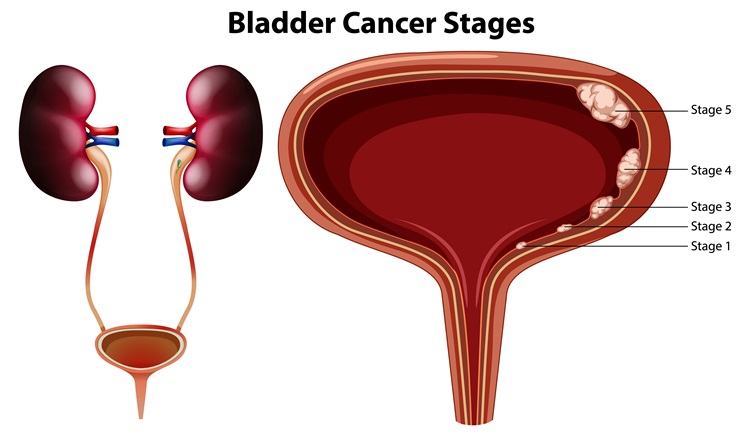
Bladder cancer is a type of cancer that begins in the cells of the bladder, a hollow, muscular organ in the lower abdomen that stores urine. It is among the more common cancers, and early detection is crucial for successful treatment.
Bladder cancer typically originates in the urothelial cells that line the inside of the bladder. It can be categorized into several types, with urothelial carcinoma (also known as transitional cell carcinoma) being the most common. Other less common types include squamous cell carcinoma and adenocarcinoma.
Several factors can increase the risk of bladder cancer, including:
Smoking: This is the most significant risk factor.
Exposure to certain chemicals: Industrial chemicals used in dyeing, rubber, leather, textiles, and paint industries.
Chronic bladder inflammation: Such as from recurrent urinary tract infections or parasitic infections.
Age: The risk increases with age.
Family history: A genetic predisposition can play a role.
Early symptoms of bladder cancer can often be subtle, making timely diagnosis important:
Hematuria (Blood in Urine): This is the most common symptom and can be visible (gross hematuria) or microscopic.
Frequent Urination: A persistent need to urinate more often than usual.
Painful Urination (Dysuria): Discomfort or burning during urination.
Urgency: A sudden, strong urge to urinate.
Back or Pelvic Pain: In more advanced stages.
Diagnosis typically involves:
Urine Tests: To check for blood, abnormal cells (cytology), and other markers.
Cystoscopy: A procedure where a thin tube with a camera is inserted into the bladder to visualize the lining.
Biopsy: Tissue samples are taken during cystoscopy for pathological examination.
Imaging Studies: CT scans, MRI, or ultrasound may be used to determine the extent of the cancer.
Treatment for bladder cancer depends on the stage, grade, and type of cancer, as well as the patient’s overall health. Options may include:
Transurethral Resection of Bladder Tumor (TURBT): A common initial procedure for early-stage bladder cancer, where the tumor is removed through the urethra.
Intravesical Therapy: Medications are instilled directly into the bladder to prevent recurrence, often after TURBT.
Cystectomy: Surgical removal of part (partial cystectomy) or all (radical cystectomy) of the bladder. If the entire bladder is removed, a urinary diversion procedure is performed.
Chemotherapy: Used before surgery to shrink tumors, after surgery to kill remaining cancer cells, or for advanced bladder cancer.
Radiation Therapy: High-energy rays are used to kill cancer cells, sometimes combined with chemotherapy.
Immunotherapy: Medications that stimulate the body’s immune system to fight cancer cells.
Targeted Therapy: Drugs that target specific weaknesses in cancer cells.
After treatment, regular follow-up care is crucial to monitor for recurrence and manage any side effects. This typically includes:
Regular Cystoscopies: To check the bladder lining.
Imaging Scans: To monitor for cancer spread.
Urine Tests: To detect any abnormal cells.
Patients are also encouraged to adopt healthy lifestyle habits and may receive support to quit smoking, which significantly reduces the risk of recurrence.
Bladder cancer is a serious condition, but with early detection and advancements in medical and surgical treatments, patients have increasingly positive outcomes. A comprehensive and personalized treatment plan, combined with diligent follow-up, is key to managing the disease and improving quality of life. Consulting with a urologist or oncologist experienced in bladder cancer is a vital step for diagnosis and treatment.

Kidney tumors are abnormal growths that develop in the kidney. While not all kidney tumors are cancerous (malignant), it is crucial to accurately diagnose and treat them due to the potential for significant health implications.
Kidney tumors can be either benign (non-cancerous) or malignant (cancerous). The most common type of kidney cancer in adults is renal cell carcinoma (RCC), which accounts for about 90% of all kidney cancers. Other types include transitional cell carcinoma, Wilms tumor (more common in children), and various benign growths like angiomyolipoma.
Several factors can increase the risk of developing kidney tumors, including:
Smoking: A significant risk factor.
Obesity: Increases the risk of RCC.
High Blood Pressure (Hypertension): Linked to an elevated risk.
Genetics and Family History: Certain inherited conditions (e.g., von Hippel-Lindau disease, Birt-Hogg-Dubé syndrome) increase risk.
Advanced Kidney Disease or Dialysis: Patients on long-term dialysis have a higher risk.
Exposure to certain substances: Such as cadmium or asbestos.
Kidney tumors often do not cause symptoms in their early stages and are frequently discovered incidentally during imaging tests for other conditions. When symptoms do appear, they can include:
Hematuria (Blood in Urine): Visible or microscopic blood in the urine.
Persistent Back or Side Pain: A dull ache not related to injury.
A Lump or Mass in the Side or Abdomen: May be palpable in some cases.
Unexplained Weight Loss.
Fatigue.
Fever that is not due to an infection.
Diagnosis typically involves:
Imaging Tests:
Ultrasound: Often the first test to detect a mass.
CT Scan (Computed Tomography): Provides detailed images and helps determine the size and extent of the tumor.
MRI (Magnetic Resonance Imaging): Used in specific cases, especially for those who cannot receive CT contrast or for further characterization.
Urine Tests: To check for blood and other abnormalities.
Blood Tests: To assess kidney function and general health.
Biopsy: While not always necessary, a needle biopsy can sometimes be performed to confirm whether a tumor is cancerous, especially if the treatment plan might change based on the pathology.
Treatment for kidney tumors depends on several factors, including the type, size, stage of the tumor, and the patient’s overall health and kidney function. Options may include:
Surgery:
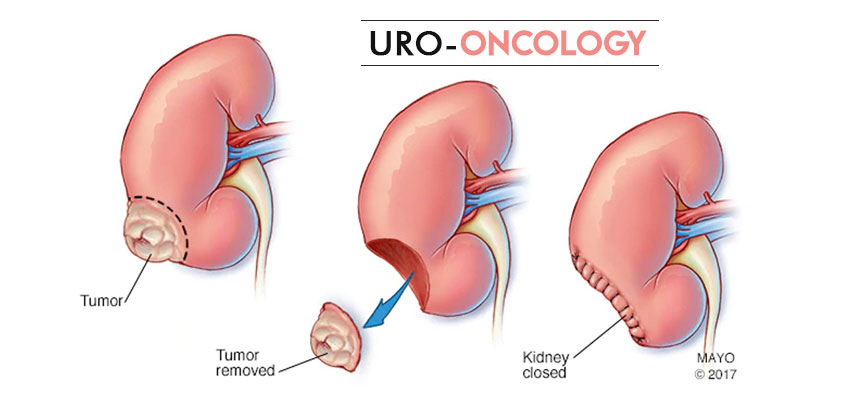
Partial Nephrectomy: Removal of only the tumor and a small margin of healthy kidney tissue, preserving the rest of the kidney. This is often preferred for smaller tumors.
Radical Nephrectomy: Removal of the entire kidney, often along with the adrenal gland and surrounding lymph nodes.
Ablation Techniques: For small tumors, these minimally invasive procedures destroy cancer cells without removing them.
Radiofrequency Ablation (RFA): Uses heat to destroy tumor cells.
Cryoablation: Uses extreme cold to freeze and destroy tumor cells.
Active Surveillance: For very small, slow-growing tumors, especially in older patients or those with other significant health issues, watchful waiting with regular imaging may be an option.
Targeted Therapy: Medications that specifically target cancer cells by interfering with their growth signals.
Immunotherapy: Drugs that boost the body’s own immune system to fight cancer cells.
Radiation Therapy: Less commonly used for primary kidney tumors but can be an option for pain relief or when cancer has spread to other areas.
Chemotherapy: Generally not highly effective for renal cell carcinoma but may be used for certain rare types of kidney cancer.
After treatment for a kidney tumor, regular follow-up care is essential to monitor for recurrence and manage any potential side effects. This typically includes:
Regular Imaging Scans: To check for new tumors or recurrence.
Blood and Urine Tests: To monitor kidney function and overall health.
Patients are encouraged to adopt a healthy lifestyle, including maintaining a healthy weight, controlling blood pressure, and quitting smoking, to promote overall well-being and reduce the risk of future health issues.
Kidney tumors can range from benign to aggressive cancers, making accurate diagnosis and personalized treatment critical. With advancements in diagnostic imaging and a wide array of treatment options, many patients achieve positive outcomes. Consulting with a urologist or oncologist experienced in kidney cancer is a vital step for effective diagnosis, treatment planning, and long-term care.
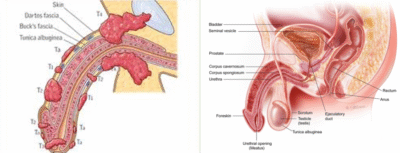
Penile cancer is a rare type of cancer that begins on or in the penis. While uncommon, it is a serious condition that requires prompt attention and specialized care.
Penile cancer typically originates in the skin cells of the penis, most often on the foreskin or glans (head of the penis). It is classified based on the type of cell where the cancer begins, with squamous cell carcinoma being the most prevalent form. Other rarer types include melanoma, basal cell carcinoma, and sarcoma.
Several factors can increase the risk of developing penile cancer:
Human Papillomavirus (HPV) Infection: Certain high-risk strains of HPV are strongly linked to penile cancer.
Phimosis: A condition where the foreskin cannot be fully retracted, leading to chronic inflammation and poor hygiene.
Poor Hygiene: Inadequate cleaning under the foreskin can contribute to chronic irritation.
Smoking: Tobacco use is a significant risk factor for many cancers, including penile cancer.
Age: The risk increases with age, most commonly affecting men over 60.
Psoriasis Treatment: Men treated with psoralen and ultraviolet A (PUVA) light therapy for psoriasis may have an increased risk.
Early detection of penile cancer is critical for effective treatment and better outcomes. Symptoms can include:
Skin Changes: A lump, sore, rash, or growth on the penis that does not heal.
Color Changes: Redness, discoloration, or thickening of the skin of the penis.
Discharge: Foul-smelling discharge under the foreskin.
Bleeding: Bleeding from the penis or under the foreskin.
Swelling: Swelling at the end of the penis.
Pain: Pain in the penis, though often absent in early stages.
Diagnosis typically involves:
Physical Examination: A thorough examination of the penis and groin area.
Biopsy: A small tissue sample is taken from the suspicious area for microscopic examination to confirm the presence of cancer cells and determine the type and grade.
Imaging Studies: MRI, CT scans, or ultrasound may be used to determine the extent of the cancer and if it has spread to lymph nodes or other parts of the body.
Treatment for penile cancer depends on the stage, size, and location of the tumor, as well as the patient’s overall health. Treatment aims to remove the cancer while preserving as much penile function and appearance as possible. Options may include:
Local Treatments (for early-stage superficial cancers):
Topical Chemotherapy/Immunotherapy: Creams applied directly to the skin.
Laser Ablation: Using a laser to destroy cancer cells.
Cryotherapy: Freezing cancer cells.
Mohs Surgery: A specialized technique to remove thin layers of skin containing cancer cells.
Surgery:
Excisional Surgery: Removing the tumor and a margin of healthy tissue.
Glansectomy: Removal of the glans (head) of the penis.
Partial or Total Penectomy: Removal of part or all of the penis for more advanced cancers.
Lymphadenectomy: Surgical removal of lymph nodes in the groin if cancer has spread (this may include Robotic VEIL Surgery for a minimally invasive approach).
Radiation Therapy: High-energy rays are used to kill cancer cells, sometimes combined with chemotherapy.
Chemotherapy: Used for advanced penile cancer that has spread to other parts of the body.
After treatment, regular follow-up care is essential to monitor for recurrence, manage side effects, and support the patient’s physical and emotional well-being. This may include:
Regular Physical Examinations: Of the penis and groin.
Imaging Scans: To monitor for any signs of recurrence or spread.
Counseling and Support: To address body image concerns, sexual health, and psychological impact.
Patients are also encouraged to maintain good penile hygiene and may receive advice on HPV vaccination to reduce future risks.
Penile cancer, though challenging, can be effectively treated, especially when diagnosed early. With advancements in surgical techniques and a multidisciplinary approach to care, the goal is to eradicate the cancer while preserving quality of life. Consulting with a urologist or oncologist specializing in penile cancer is a crucial step for accurate diagnosis and personalized treatment planning.
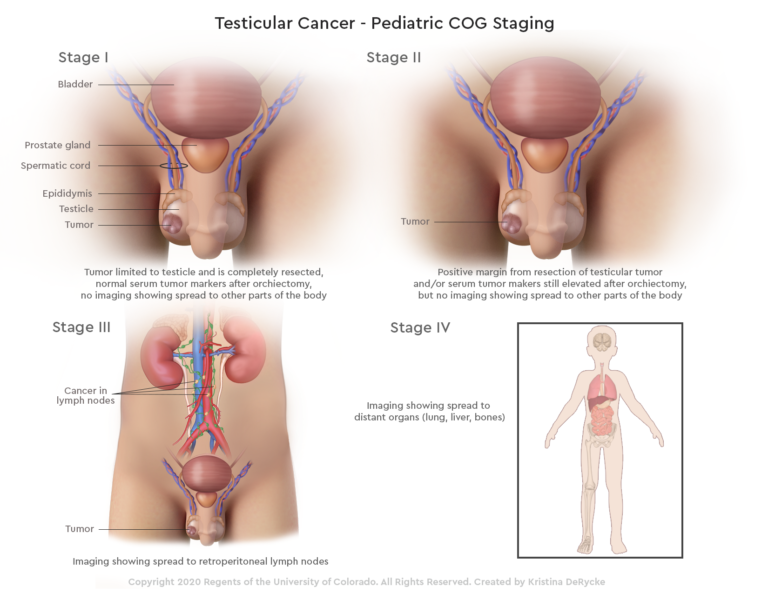
Testicular tumors, though relatively rare, are the most common cancer in males aged 15 to 49. Early detection and prompt treatment are crucial for achieving high cure rates.
Testicular tumors are abnormal growths that develop in one or both testicles. The vast majority of these tumors (about 95%) are germ cell tumors, which originate in the sperm-producing cells of the testicles. These can be further classified into:
Seminomas: Grow and spread more slowly.
Non-seminomas: Tend to grow and spread more quickly.
Other, much rarer types of testicular tumors include stromal tumors (e.g., Leydig cell tumors, Sertoli cell tumors) and lymphomas.
While the exact cause of testicular cancer is unknown, several factors can increase the risk:
Cryptorchidism (Undescended Testicle): The most significant risk factor, even if corrected surgically.
Family History: A father or brother with testicular cancer.
Personal History: Having cancer in one testicle increases the risk of it occurring in the other.
Race: White men are at a higher risk than men of other races.
Age: Most common in young and middle-aged men.
The most common symptom of a testicular tumor is a lump or swelling in one of the testicles. Other symptoms may include:
A painless lump or swelling in either testicle. This is often the first sign.
A feeling of heaviness in the scrotum.
A dull ache in the abdomen or groin.
Sudden collection of fluid in the scrotum (hydrocele).
Pain or discomfort in a testicle or the scrotum.
Breast tenderness or growth: Due to hormone production by some tumors.
Diagnosis typically involves:
Physical Examination: A thorough examination of the testicles, groin, and abdomen by a doctor.
Scrotal Ultrasound: This imaging test uses sound waves to create detailed images of the testicles and can differentiate between a solid tumor and a fluid-filled cyst.
Blood Tests: To measure tumor markers such as Alpha-fetoprotein (AFP), Human Chorionic Gonadotropin (HCG), and Lactate Dehydrogenase (LDH). Elevated levels can indicate testicular cancer and help determine the type.
Biopsy: Unlike most cancers, a biopsy is rarely performed directly on the testicle if cancer is suspected, as it risks spreading cancer cells. Diagnosis is usually confirmed after surgical removal of the testicle.
Treatment for testicular tumors depends on the type, stage, and spread of the cancer, as well as the patient’s overall health. The primary treatment usually involves surgery.
Radical Inguinal Orchiectomy: This is the initial and most crucial step, involving the surgical removal of the affected testicle through an incision in the groin.
Retroperitoneal Lymph Node Dissection (RPLND): If cancer has spread to lymph nodes in the abdomen, this surgery may be performed to remove them. It can be performed traditionally or minimally invasively using robotic assistance.
Chemotherapy: Used to kill remaining cancer cells, prevent recurrence, or treat cancer that has spread to other parts of the body.
Radiation Therapy: More commonly used for seminoma, radiation may be directed at lymph nodes to kill cancer cells.
Surveillance: For very early stages, watchful waiting with close monitoring (blood tests, imaging scans) may be an option after orchiectomy.
After treatment, regular follow-up care is essential to monitor for recurrence and manage any long-term side effects. This typically includes:
Regular Physical Exams:
Blood Tests for Tumor Markers:
Imaging Scans (CT scans):
Discussions about fertility preservation: Before treatment, as some treatments can affect fertility.
Prosthetic Testicle: Many men opt for a saline-filled testicular prosthesis for cosmetic reasons.
Testicular tumors, though a serious diagnosis, are highly treatable, especially when detected early. Advances in diagnosis and treatment mean that most men with testicular cancer can expect a full recovery. Awareness of symptoms, regular self-examinations, and prompt consultation with a urologist are vital steps toward effective management and a healthy future.
Dr. Rohit Kaushal is a leading Urologist and Robotic Surgeon in Delhi, specializing in kidney transplant, prostate, and reconstructive urology with compassionate patient care.
© 2025 Created with Digital Growth Well