Optical Internal Urethrotomy (OIU) is a minimally invasive surgical procedure performed to treat urethral stricture disease, a condition where the urethra (the tube that carries urine from the bladder out of the body) becomes narrowed or blocked due to scar tissue formation.
This narrowing can lead to difficulty in urination, reduced urine flow, or recurrent urinary tract infections. OIU helps restore the normal flow of urine and relieve urinary symptoms effectively.
Optical Internal Urethrotomy is typically recommended for patients who have:
Short-segment urethral strictures (usually less than 1–2 cm)
Single, non-complex strictures
Strictures located in the bulbar urethra
Recurrence after previous urethrotomy or dilation
Common causes leading to urethral stricture formation include:
Trauma: Injury to the perineum or pelvis, often due to falls, accidents, or catheterization.
Infection: Recurrent urinary tract infections or sexually transmitted infections (e.g., gonorrhea).
Instrumentation: Prior urological procedures involving catheter or endoscopic instruments.
Inflammation: Conditions like lichen sclerosus or chronic urethritis.
Post-surgical Scarring: Following prostate or urethral surgeries.
OIU is performed under regional or general anesthesia using a urethrotome — a special endoscopic instrument with a fine blade and optical lens.
Steps involved include:
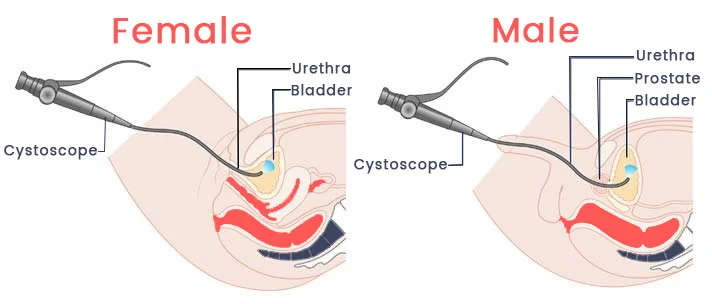
Insertion of Endoscope: The surgeon gently inserts the endoscope through the urethra to visualize the stricture.
Identification of Stricture: The exact site and extent of narrowing are identified under direct vision.
Incision: A small incision is made at the 12 o’clock position of the stricture using a cold knife or laser to open the blocked area.
Catheter Placement: After the incision, a urinary catheter is placed to keep the urethra open during healing (typically for 7–14 days).
The entire procedure usually takes 15–30 minutes and does not require any external incision.
After surgery, patients are monitored for urinary flow and comfort.
Post-surgery instructions include:
Keeping the catheter in place as advised.
Drinking plenty of fluids to flush the urinary tract.
Taking prescribed antibiotics to prevent infection.
Avoiding strenuous activities until recovery is complete.
A follow-up uroflowmetry or cystoscopy may be scheduled to assess urethral healing and ensure proper urine flow.
Minimally invasive procedure
Quick recovery time
No external scars
Effective symptom relief
Can be repeated if necessary
While OIU is generally safe, some possible risks include:
Bleeding or infection
Temporary burning during urination
Recurrence of urethral stricture
Rarely, urinary retention or incontinence
Regular follow-up with your urologist is essential to monitor for recurrence and maintain long-term results
Optical Internal Urethrotomy (OIU) is a simple and effective treatment for short urethral strictures.
With early diagnosis, proper surgical technique, and regular follow-up, most patients experience excellent outcomes and significant improvement in urinary function.
If you are facing difficulty in urination or have symptoms of a urethral blockage, consult a qualified urologist to determine if OIU is the right treatment for you.
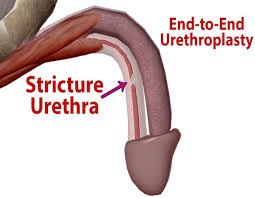
End-to-End Urethroplasty is a surgical procedure performed to treat urethral strictures, especially when the narrowed segment is short and dense. This technique involves the complete excision of the scarred urethral segment and direct reconnection (anastomosis) of the healthy urethral ends, restoring normal urine flow.
End-to-End Urethroplasty is typically recommended for patients with:
Short-segment urethral strictures (usually less than 2 cm)
Dense scar tissue not responsive to dilation or internal urethrotomy
Recurrent urethral strictures after previous treatments
Strictures located in the bulbar or penile urethra suitable for tension-free anastomosis
Common causes leading to urethral strictures include:
Trauma: Pelvic fractures, straddle injuries, or instrumentation-related trauma.
Infection: Chronic urinary tract infections or sexually transmitted infections.
Inflammatory Disorders: Conditions like lichen sclerosus.
Post-Surgical Scarring: After prior urological surgeries or catheterizations.
End-to-End Urethroplasty is performed under general or regional anesthesia.
Steps involved include:
Exposure of Stricture: The urethra is surgically exposed through a perineal or penile incision.
Excision of Scar Tissue: The diseased segment of the urethra is completely removed.
Spatulated Anastomosis: The healthy urethral ends are carefully spatulated and reconnected to ensure a wide, tension-free urethral lumen.
Catheter Placement: A urinary catheter is placed to support healing and maintain urethral patency.
The procedure is precise and typically requires 2–3 hours, depending on stricture complexity.
After surgery, careful follow-up is essential to ensure proper healing.
Post-surgery instructions include:
Keeping the catheter in place as advised (usually 2–3 weeks).
Maintaining adequate hydration.
Avoiding strenuous activity or heavy lifting until cleared by the urologist.
Monitoring for signs of infection or difficulty in urination.
A retrograde urethrogram or uroflowmetry may be performed before catheter removal to confirm successful reconstruction.
High success rate for short urethral strictures
Permanent resolution of the stricture in most cases
Reduces recurrence compared to internal urethrotomy
Restores normal urinary function
Can improve quality of life and prevent complications such as urinary retention or infections
While generally safe, some possible risks include:
Bleeding or infection
Temporary urinary discomfort
Rare risk of stricture recurrence
Urinary incontinence or erectile dysfunction (rare)
End-to-End Urethroplasty is a gold-standard surgical option for short, dense urethral strictures.
With proper patient selection, skilled surgical technique, and regular follow-up, it offers excellent long-term outcomes and significantly improves urinary function.
If you are experiencing persistent difficulty in urination due to urethral narrowing, consult a qualified urologist to evaluate the suitability of this procedure.

Buccal Mucosal Urethroplasty is an advanced reconstructive surgery performed to treat long or complex urethral strictures that cannot be managed by simpler procedures such as internal urethrotomy or end-to-end urethroplasty.
This technique uses the patient’s own buccal mucosa (inner cheek lining) as a graft to reconstruct and widen the narrowed urethral segment, ensuring long-term urethral patency and improved urinary flow.
This procedure is recommended for patients with:
Long-segment urethral strictures (>2 cm)
Multiple or recurrent strictures after failed previous surgeries
Strictures caused by lichen sclerosus, infection, or trauma
Complex anterior urethral strictures where primary anastomosis is not possible
Urethral strictures can develop due to:
Trauma: Pelvic or perineal injury, falls, or catheter-related trauma.
Infections: Chronic urinary tract infections or sexually transmitted infections (STIs).
Iatrogenic Causes: Repeated instrumentation or prior urethral surgeries.
Inflammatory Disorders: Conditions such as lichen sclerosus.
Post-surgical Scarring: After prostate or penile surgeries.
The surgery is performed under general anesthesia and involves two main stages — graft harvesting and urethral reconstruction.
Steps involved include:
Graft Harvesting: A thin layer of mucosa is carefully taken from the inside of the cheek (buccal mucosa). This tissue is ideal for grafting due to its thick epithelium and resistance to infection.
Stricture Exposure: The diseased portion of the urethra is exposed through a perineal incision.
Graft Placement: The harvested mucosal graft is sutured to the opened segment of the urethra (onlay technique) to reconstruct and widen the narrowed area.
Catheterization: A urinary catheter is inserted to support healing and maintain urethral alignment.
The cheek area typically heals quickly without noticeable scarring or functional issues.
Proper postoperative management is essential for successful recovery.
After surgery:
The catheter is usually kept in place for 2–3 weeks.
Mouth rinses are prescribed to maintain oral hygiene and promote cheek healing.
Adequate fluid intake is encouraged.
Avoid spicy or hard foods for the first few days to reduce oral discomfort.
Physical activity should be limited until the urethra heals completely.
Follow-up tests such as urethrograms or uroflowmetry are conducted to ensure the urethra remains open and functional.
Excellent long-term success rate (80–90%)
Uses patient’s own tissue, minimizing rejection risk
Suitable for long and complex strictures
Durable and resistant to infection
Restores normal urinary flow and quality of life
Though generally safe, possible complications may include:
Mild oral discomfort or numbness (temporary)
Bleeding or infection at the surgical site
Recurrent urethral stricture (rare)
Fistula formation or narrowing at the anastomotic site (uncommon)
Regular follow-up with your urologist helps detect and manage any complications early.
Buccal Mucosal Urethroplasty is a highly effective and durable surgical technique for complex urethral strictures.
By using the patient’s own cheek lining, it provides a natural and long-lasting repair with minimal side effects.
If you are suffering from recurrent or long-segment urethral narrowing, consult a qualified urologist to discuss whether Buccal Mucosal Urethroplasty is the right option for you.
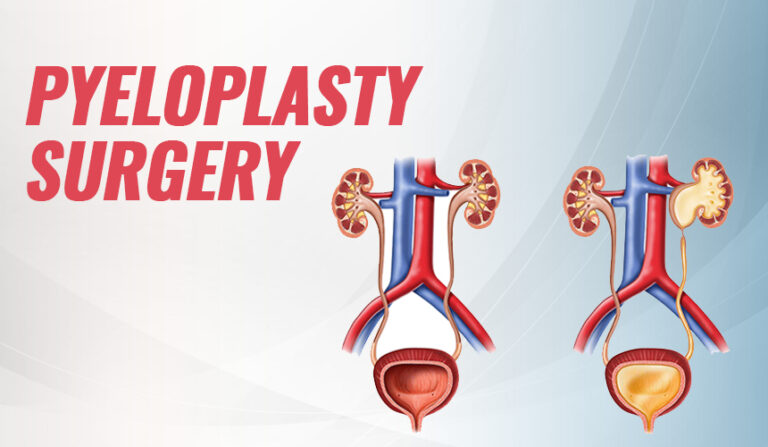
Pyeloplasty is a surgical procedure performed to correct ureteropelvic junction (UPJ) obstruction, a condition in which the connection between the kidney’s renal pelvis and the ureter becomes narrowed or blocked.
This blockage prevents normal urine drainage from the kidney to the bladder, leading to pain, infection, or kidney damage. Pyeloplasty restores proper urine flow and helps preserve kidney function.
Pyeloplasty is recommended for patients with:
Congenital or acquired UPJ obstruction
Flank pain or recurrent urinary tract infections
Hydronephrosis (swelling of the kidney due to urine buildup)
Decreased kidney function due to obstruction
Recurrent stones in the renal pelvis
Common causes include:
Congenital Narrowing: Present since birth due to abnormal muscle development or crossing vessels.
Scar Tissue: Resulting from previous surgery, infection, or trauma.
Crossing Blood Vessels: An artery or vein crossing the ureter can compress the junction.
Infection or Inflammation: Chronic infections causing fibrosis or narrowing.
Postoperative Changes: Following prior urological procedures.
Pyeloplasty can be performed through open, laparoscopic, or robot-assisted techniques, depending on the patient’s condition.
Steps involved include:
Exposure: The affected kidney and ureter are carefully exposed.
Excision: The obstructed segment at the ureteropelvic junction is removed.
Reconstruction: The healthy end of the ureter is reattached to the renal pelvis (known as Anderson-Hynes dismembered pyeloplasty).
Stenting: A temporary ureteric stent is placed to ensure smooth urine drainage during healing.
The procedure typically lasts 2–3 hours, and patients usually recover within a few days after surgery
Postoperative recovery includes:
Keeping the ureteric stent in place for 4–6 weeks (removed later via cystoscopy).
Adequate hydration to maintain urine flow.
Avoiding strenuous activity for a few weeks.
Regular follow-up ultrasounds or scans to assess kidney drainage and function.
Restores normal urine drainage from the kidney
Relieves pain and infection risk
Prevents progressive kidney damage
High long-term success rate (>90%)
Can be performed with minimally invasive (laparoscopic/robotic) techniques
Though generally safe, potential complications include:
Bleeding or infection
Urine leakage from the repair site
Recurrence of obstruction (rare)
Stent-related discomfort or infection
Prompt follow-up ensures early detection and management of any issues.
Pyeloplasty is a safe and effective surgical solution for treating ureteropelvic junction obstruction and restoring healthy kidney function.
With modern minimally invasive techniques, patients experience faster recovery, less pain, and excellent long-term outcomes.
If you have symptoms of kidney blockage such as flank pain, infection, or hydronephrosis, consult a qualified urologist to evaluate whether Pyeloplasty is the right treatment for you.
Boari’s Flap is a reconstructive urological surgery performed to repair defects or strictures of the lower or mid-ureter, particularly when a direct reimplantation of the ureter into the bladder is not possible due to a long ureteric defect.
This technique uses a flap of the bladder wall (Boari’s flap) to bridge the gap between the ureter and bladder, thereby restoring the normal passage of urine from the kidney to the bladder.
Boari’s Flap ureteral reconstruction is typically indicated in cases such as:
Long-segment lower ureteric strictures or injuries
Ureteric damage due to prior pelvic surgery or radiation
Ureteral avulsion or ischemia following stone removal procedures
Failed previous ureteric reimplant surgeries
Iatrogenic ureteral injuries during gynecological or colorectal operations
Common causes include:
Surgical Trauma: During hysterectomy, pelvic surgery, or colorectal operations.
Ureteric Stones: Long-standing impacted stones causing scarring.
Infections: Chronic urinary infections leading to fibrosis.
Radiation Injury: Pelvic radiotherapy resulting in ischemic strictures.
Accidental Injury: During endoscopic or ureteric interventions.
Boari’s Flap is performed under general anesthesia and may be done through open, laparoscopic, or robotic-assisted techniques.
Steps involved include:
Mobilization of the Bladder: The bladder is mobilized to provide adequate reach to the damaged ureter.
Creation of the Flap: A rectangular flap of bladder wall is raised while preserving its blood supply.
Tubularization: The flap is folded and sutured to form a tubular structure resembling the ureter.
Anastomosis: The tubularized flap is connected to the healthy upper ureteral segment, creating a tension-free, watertight junction.
Stent Placement: A temporary ureteric stent is inserted to ensure proper drainage during healing.
The technique effectively bridges long ureteric defects up to 12–15 cm in length.
Post-surgery, careful management and follow-up are essential for successful recovery.
Care instructions include:
Maintaining adequate hydration.
Keeping the ureteric stent in place for 4–6 weeks.
Avoiding heavy lifting or strenuous activity until healing is complete.
Regular imaging (ultrasound or CT urography) to assess urine flow and kidney function.
Monitoring for urinary infections or discomfort.
Restores normal urinary drainage in long ureteric defects
Uses the patient’s own bladder tissue, reducing rejection risk
High success rate with durable outcomes
Can be performed with minimally invasive surgical techniques
Preserves kidney function and prevents hydronephrosis
Although Boari’s Flap is a safe and established procedure, potential risks may include:
Urinary leakage from the anastomosis site
Infection or hematuria
Stent-related discomfort
Bladder spasms or temporary frequency
Rarely, recurrence of obstruction or stricture
Close follow-up ensures timely detection and management of any postoperative complications.
Boari’s Flap is an effective reconstructive option for patients with long lower or mid-ureteric strictures where direct reimplantation is not feasible.
By utilizing a flap of the patient’s own bladder tissue, the procedure provides a reliable and long-term solution for restoring urinary continuity and preserving kidney function.
If you are diagnosed with ureteric stricture or injury, consult a qualified urologist to determine if Boari’s Flap reconstruction is the most suitable treatment for you.
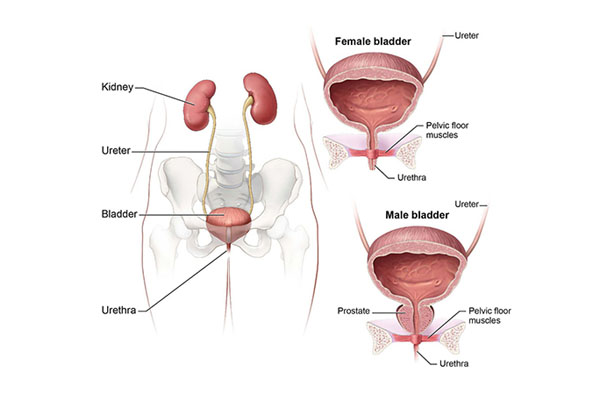
Ureteric Reimplantation (or Ureteral Reimplantation) is a surgical procedure performed to correct abnormalities or treat conditions affecting the ureters—the tubes that carry urine from the kidneys to the bladder. This procedure is primarily used to restore the proper flow of urine and protect the kidneys from damage.
Ureteric reimplantation is a surgical intervention designed to correct a faulty connection where the ureter enters the bladder. The most common indication for this surgery is Vesicoureteral Reflux (VUR), a condition where urine flows backward from the bladder into the ureters and potentially up to the kidneys. This backflow can lead to recurrent urinary tract infections (UTIs) and, if left untreated, cause kidney damage.
The surgery corrects this issue by:
Creating a new, more effective connection between the ureter and the bladder.
Creating a new tunnel within the bladder wall that mimics the natural valve-like mechanism. This new positioning ensures that the bladder muscle compresses the ureter during urination, preventing backflow (reflux).
Ureteric reimplantation is a highly effective treatment that offers significant benefits, especially in cases of VUR and ureteral obstruction:
Prevents Kidney Damage: By stopping the backflow of urine (reflux), the procedure protects the kidneys from ascending infections and potential long-term scarring or damage.
Effective Symptom Relief: It effectively alleviates the risk of recurrent urinary tract infections caused by VUR.
High Success Rate: The operation has a very high success rate in correcting the faulty connection and preventing future reflux.
Treatment for Obstruction: It is also used to correct narrowing or blockage at the junction between the ureter and the bladder (VUJ obstruction), restoring normal urine drainage.
Ureteric reimplantation is performed under general anesthesia and typically takes about two to three hours, depending on whether one (unilateral) or both (bilateral) ureters are being reimplanted.
The procedure can be performed using different techniques:
Open Surgery: Involves a small incision, often in the lower abdomen (bikini line incision).
Laparoscopic/Robotic Surgery: Minimally invasive approaches using small incisions, a camera, and specialized instruments, often providing enhanced precision and potentially quicker recovery.
During the surgery, the surgeon will:
Detach the ureter from its original position on the bladder.
Create a new tunnel within the bladder wall and reposition the ureter into this new, better-positioned tunnel.
Stitch the ureter into place to secure the new, effective connection.
A catheter (flexible drainage tube) is usually left in the bladder for a short period to drain urine and allow for healing. A temporary ureteral stent may also be placed internally to ensure proper drainage from the kidney to the bladder.
Post-procedure, patients typically stay in the hospital for 1 to 3 days. The total recovery period usually lasts 4 to 6 weeks.
Patients may temporarily experience:
Temporary Urinary Symptoms: Increased frequency and urgency in urination, or mild discomfort/burning (dysuria) due to bladder healing. Bladder spasms may occur and can be managed with prescribed medication.
Blood in Urine: It is normal for the urine to be blood-tinged (pink to light red) for a few days to a few weeks, particularly if a stent is in place.
Patients are advised to:
Stay Hydrated: Drink plenty of fluids to encourage the urinary system to flush.
Restrict Activity: Avoid heavy lifting and strenuous activities, including sports and vigorous exercise, for approximately 4 to 6 weeks or as advised by the urologist, to prevent strain on the surgical site.
Manage Pain: Pain and discomfort will be managed with prescribed medication.
Follow-up: Regular follow-up appointments, including imaging tests (like ultrasound or a Voiding Cystourethrogram/VCUG) 4-6 weeks post-surgery, are crucial to monitor healing and confirm the success of the procedure.
While Ureteric Reimplantation is a safe and effective procedure, thorough consultation with your urologist is essential to determine the best surgical approach tailored to your (or your child’s) specific condition and medical history.
It is an anatomical reconstruction that involves creating a new connection between the ureter (the tube that carries urine from the kidney to the bladder) and one of the kidney’s calyces (a cup-like part of the kidney’s urine-collecting system).
Ureterocalycostomy is typically considered a salvage or rescue procedure when more common reconstructive surgeries, like pyeloplasty, have failed or are not possible due to complex anatomical issues. The primary goal is to restore continuous, non-obstructed urine flow and preserve kidney function.
It is generally indicated for patients with:
Failed Pyeloplasty (Redo Surgery): This is one of the most common reasons, particularly when previous surgeries have caused severe scarring (fibrosis) around the ureteropelvic junction (UPJ), which is the area where the renal pelvis connects to the ureter.
Complex Ureteropelvic Junction Obstruction (UPJO): Conditions that make standard repair difficult, such as:
An intrarenal pelvis (where the main urine-collecting structure is completely within the kidney).
A short ureter length.
Congenital anomalies like a malrotated kidney.
Long Proximal Ureteral Strictures: Scarring or narrowing in the upper part of the ureter, often due to previous surgery (like for kidney stones) or diseases like tuberculosis.
Other Obstructions or Injuries: In specific cases of trauma or post-surgical complications where the renal pelvis is scarred or the proximal ureter is severely damaged.
The procedure generally involves:
Disconnection: The diseased or obstructed connection between the ureter and the renal pelvis is severed.
Access: A portion of the lower pole of the kidney is surgically removed (lower pole amputation) to gain wide access to the lowest calyx (the inferior calyx). This ensures good, dependent drainage.
Anastomosis: The healthy end of the ureter is meticulously sewn to the opened lower pole calyx. This is a crucial step that aims for a wide, tension-free connection to prevent future scarring.
Stenting: A temporary ureteral stent (a small tube) is often placed to ensure proper healing and guide urine flow during recovery.
The surgery can be performed through an open incision (traditional) or using minimally invasive techniques like laparoscopy or robot-assisted surgery.
Recovery will vary based on the surgical approach and the patient’s overall health, but generally involves:
Hospital Stay: Typically several days.
Post-operative Drainage: A surgical drain may be in place, and a ureteral stent will be in place for several weeks to months to protect the new connection.
Activity: Strenuous activity and heavy lifting are restricted for a period to allow the internal and external wounds to heal.
Follow-up: Regular follow-up appointments and imaging studies (like ultrasounds or renal scans) are essential to ensure the new connection is draining effectively and kidney function is stable.
Ileal Interposition is a specialized reconstructive surgical technique used to restore the continuity of the urinary tract when a segment of the ureter (the tube carrying urine from the kidney to the bladder) is damaged, diseased, or needs to be removed. This procedure is particularly valuable when the affected ureteral segment is too long to be repaired by simpler methods.
In Ileal Interposition, a small segment of the ileum (the final part of the small intestine) is isolated and used to replace or bypass the diseased portion of the ureter. The isolated bowel segment acts as a substitute ureter, maintaining urine flow from the kidney to the bladder.
This technique is indicated in cases where:
A long segment of the ureter is strictured, damaged, or removed.
Previous surgical repairs (such as ureteric reimplant or Boari’s flap) are not feasible.
The patient has sustained traumatic injury, iatrogenic damage, or severe fibrosis due to infection, stones, or radiation.
Ileal Interposition may be recommended for patients with:
Long ureteric strictures or complete ureteric loss
Ureteric injury following previous pelvic or abdominal surgery
Radiation-induced ureteral damage
Recurrent ureteric obstruction or scarring
Complex reconstructive needs after tumor resection
Restores Urinary Continuity:
Provides an effective way to re-establish the connection between the kidney and bladder when other options are not viable.
Preserves Kidney Function:
By ensuring proper urinary drainage, the procedure helps preserve the affected kidney’s function.
Durable and Reliable:
Offers long-term success with good functional outcomes and minimal risk of recurrence of obstruction.
Versatile Application:
Can be used for both unilateral and bilateral ureteral replacement, depending on the patient’s condition.
During Ileal Interposition, the surgeon selects an appropriate segment of the ileum and isolates it while maintaining its blood supply.
The diseased ureteral segment is excised, and the ileal segment is interposed between the renal pelvis (or remaining ureter) and the urinary bladder.
The two ends are connected using fine sutures to ensure a watertight and tension-free anastomosis. The bowel continuity is then restored. The entire procedure is performed under general anesthesia and may take several hours depending on the complexity of the case.
After surgery, patients are closely monitored for urine output and kidney function. Postoperative care includes:
Adequate hydration to maintain good urine flow.
Regular monitoring of renal parameters and electrolytes.
Temporary urinary drainage via stents or catheters to support healing.
Follow-up imaging to assess the integrity of the urinary tract.
Most patients can resume normal activities gradually as recovery progresses, under the guidance of their urologist.
While Ileal Interposition is an effective and durable solution, it is a complex procedure and must be carefully considered.
Factors such as overall health, renal function, previous surgeries, and the length of ureteral loss influence surgical planning and outcomes.
A detailed evaluation and discussion with a qualified urologic surgeon are essential before proceeding with this reconstructive option.
Renal Autotransplant (also known as Kidney Autotransplantation) is a highly specialized surgical procedure used in complex urological and vascular conditions to preserve kidney function when conventional surgical options are not feasible. This advanced reconstructive technique involves removing a patient’s own kidney and reimplanting it into a different location within the body to restore or improve urinary drainage and blood flow.
In Renal Autotransplant, the kidney is surgically removed from its original position and reimplanted—usually into the pelvic region—where the blood vessels and ureter are reconstructed to re-establish normal function.
The procedure allows the surgeon to manage complex conditions involving the ureter, renal artery, or renal pelvis, while preserving the kidney rather than removing it.
Renal Autotransplant is typically recommended in the following situations:
Complex or long ureteric strictures where standard reconstruction (like Boari’s flap or ileal interposition) is not possible
Renal artery aneurysms or other vascular abnormalities of the kidney
High ureteric injury resulting from trauma or previous surgeries
Tumors or lesions near the renal hilum that require precise surgical access
Renal artery stenosis not suitable for angioplasty or stenting
Chronic ureteric obstruction with preserved kidney function
Preserves Native Kidney Function:
Allows the kidney to be salvaged and continue functioning, avoiding the need for nephrectomy (kidney removal).
Restores Urinary and Vascular Continuity:
Enables effective reconstruction of the ureter or renal vessels in complex cases.
Improved Access and Precision:
Relocating the kidney to the pelvic region offers better surgical exposure for vascular and ureteric repair.
Long-Term Success:
Provides durable outcomes with good preservation of renal function and relief from symptoms.
During Renal Autotransplant, the surgeon carefully removes the kidney, preserving its blood vessels and ureter.
Outside the body, the kidney may undergo necessary repair of the ureter, renal artery, or renal pelvis.
The kidney is then reimplanted into the iliac fossa (pelvic region)—similar to the placement of a donor kidney in a transplant surgery.
The renal artery and vein are connected to the iliac vessels, and the ureter is attached to the urinary bladder.
Once blood flow is restored, the kidney begins functioning again in its new location.
The procedure is performed under general anesthesia and typically lasts several hours, depending on the complexity of the case.
After surgery, patients are closely monitored for:
Kidney function (urine output and creatinine levels)
Blood flow to the transplanted kidney via imaging
Fluid balance and hydration
Signs of infection or complications
Temporary stents or catheters may be placed to aid healing of the urinary connection. Most patients recover over a few weeks and gradually return to normal activities under medical supervision.
Renal Autotransplant represents a remarkable advancement in reconstructive and vascular urology.
It provides an opportunity to preserve kidney function and restore normal urinary and vascular anatomy in patients with otherwise inoperable conditions.
With expert surgical care and comprehensive postoperative management, renal autotransplantation offers excellent long-term results and improved quality of life for selected patients.
Dr. Rohit Kaushal is a leading Urologist and Robotic Surgeon in Delhi, specializing in kidney transplant, prostate, and reconstructive urology with compassionate patient care.
© 2025 Created with Digital Growth Well