Recurrent Urinary Tract Infection (UTI) is a common and distressing condition that affects many women worldwide. It is defined as having two or more infections within six months or three or more infections within a year. Recurrent UTIs can significantly impact quality of life, causing discomfort, anxiety, and disruption to daily activities. Understanding the underlying causes, risk factors, and available treatment options is essential for effective management and prevention.
Recurrent UTIs occur when bacteria repeatedly enter and infect the urinary tract. The most common bacteria responsible are Escherichia coli (E. coli), which normally reside in the intestinal tract.
Incomplete Bladder Emptying: Retention of urine can promote bacterial growth.
Sexual Activity: Frequent sexual intercourse can introduce bacteria into the urinary tract.
Use of Spermicides or Diaphragms: These can alter vaginal flora, increasing infection risk.
Menopause: Decreased estrogen levels can lead to thinning of the vaginal tissues and reduced natural protection against bacteria.
Genetic or Anatomical Factors: Some women are more prone due to structural differences in the urinary tract.
Poor Hygiene Practices: Incorrect wiping or delayed urination can allow bacterial spread.
The symptoms of recurrent UTI are similar to those of a single urinary tract infection, but they occur repeatedly over time.
Burning sensation during urination
Increased frequency and urgency to urinate
Lower abdominal or pelvic pain
Cloudy or foul-smelling urine
Blood in urine (hematuria)
General discomfort or fatigue
Accurate diagnosis is key to proper management and prevention of further infections. Your urologist will review your medical history and may recommend specific tests to identify the cause.
Diagnostic Tools May Include:
Urine Analysis and Culture: To detect bacteria and identify the most effective antibiotics.
Ultrasound or CT Scan: To check for anatomical abnormalities, stones, or obstruction.
Cystoscopy: A small camera inserted into the bladder to examine for inflammation or structural issues.
Post-Void Residual Test: To evaluate if urine remains in the bladder after urination.
The treatment approach for recurrent UTI depends on the frequency, severity, and underlying cause of infection.
Short-Course Antibiotics: For active infections.
Prophylactic Antibiotics: Low-dose, long-term antibiotics may be prescribed in chronic cases.
In postmenopausal women, topical estrogen creams or tablets help restore healthy vaginal flora and reduce recurrence.
Increase water intake to flush out bacteria.
Urinate before and after sexual activity.
Maintain proper genital hygiene.
Avoid irritants such as harsh soaps, douches, or powders.
Treatment of contributing factors like kidney stones, diabetes, or pelvic organ prolapse can reduce recurrence.
Preventing recurrent UTIs is as important as treating them.
Preventive Tips Include:
Stay well-hydrated and avoid holding urine for long periods.
Wear breathable cotton underwear and avoid tight clothing.
Maintain balanced vaginal pH and healthy flora.
Consider probiotics to support urinary and vaginal health.
Discuss preventive antibiotic or non-antibiotic regimens with your urologist if infections persist.
Seek immediate medical attention if you experience:
Frequent UTIs within a short duration
Fever, chills, or flank pain (possible kidney involvement)
Blood in urine or worsening symptoms despite treatment
Early diagnosis and prompt treatment can prevent complications such as kidney infections or chronic bladder issues.
Recurrent UTI in females is a common yet manageable condition. With accurate diagnosis, tailored treatment, and preventive care, most women can achieve long-term relief and avoid repeated infections. If you experience frequent urinary tract infections, consult a qualified urologist to determine the best course of management and prevent future recurrence.

Stress Urinary Incontinence (SUI) is a common condition characterized by the involuntary leakage of urine during physical activities that put pressure (stress) on the bladder, such as coughing, sneezing, laughing, or exercising. It is more common in women but can also affect men, especially after prostate surgery. While not life-threatening, SUI can significantly impact daily life, emotional well-being, and confidence.
Stress urinary incontinence occurs when the muscles and tissues supporting the bladder and urethra weaken, reducing their ability to control urine flow during increased abdominal pressure.
Common Causes Include:
Pregnancy and Childbirth: Vaginal delivery can stretch or weaken pelvic floor muscles and nerves.
Menopause: Decreased estrogen levels lead to thinning of the urethral and vaginal tissues.
Pelvic Surgery: Procedures like hysterectomy or prostate surgery may affect the pelvic support structures.
Obesity: Extra body weight increases pressure on the bladder.
Chronic Coughing or Constipation: Frequent straining can weaken pelvic muscles over time.
Aging: Natural muscle weakening associated with aging can contribute to SUI.
The primary symptom of SUI is the involuntary leakage of urine during physical activity or exertion.
Common Symptoms Include:
Leakage of urine during coughing, sneezing, laughing, or lifting objects
Urine leakage during exercise or sudden movement
Minimal or no leakage during sleep
No strong urgency before leakage (unlike urge incontinence)
Feelings of embarrassment or anxiety due to recurrent leakage
Lorem ipsum dolor sit amet, consectetur adipiscing elit. Ut elit tellus, luctus nec ullamcorper mattis, pulvinar dapibus leo.
Diagnostic Tools May Include:
Medical History & Physical Examination: Assessment of symptoms, triggers, and medical background.
Urinalysis: To rule out infections or other urinary abnormalities.
Bladder Diary: Recording fluid intake, urination frequency, and leakage episodes.
Urodynamic Testing: Evaluates bladder pressure, capacity, and muscle function.
Cystoscopy: Allows direct visualization of the urethra and bladder to detect any abnormalities.
Treatment for stress urinary incontinence depends on the severity of symptoms, patient preference, and underlying cause. Management may include conservative, medical, or surgical approaches.
Pelvic Floor Exercises (Kegel Exercises): Strengthen the muscles that control urination.
Weight Reduction: Reduces pressure on the bladder.
Bladder Training: Establishes regular voiding schedules.
Avoiding Bladder Irritants: Limit caffeine, alcohol, and acidic foods.
Topical Estrogen Therapy: For postmenopausal women to improve urethral tone.
Pessary Devices: Support the urethra and bladder neck in women with mild leakage.
For moderate to severe SUI, surgical options may provide long-term relief.
Common Procedures Include:
Mid-Urethral Sling Surgery: Placement of a supportive mesh tape under the urethra.
Bladder Neck Suspension: Lifts and supports the bladder neck to prevent leakage.
Urethral Bulking Agents: Injections that improve urethral closure by adding bulk to the tissues.
You should consult a urologist or urogynecologist if you experience:
Frequent urine leakage affecting daily life
Difficulty controlling bladder during physical activity
Reduced confidence or social discomfort due to leakage
Early evaluation ensures timely management and prevents worsening of symptoms.
While not all cases of SUI can be prevented, certain lifestyle changes can help reduce risk and improve bladder control.
Preventive Tips:
Perform regular pelvic floor exercises
Maintain a healthy body weight
Treat chronic cough or constipation promptly
Avoid smoking and excessive caffeine intake
Stay physically active to promote muscle strength
Stress Urinary Incontinence (SUI) is a manageable condition with several effective treatment options available. Early diagnosis and proper management can restore bladder control, improve confidence, and enhance quality of life. If you experience urine leakage during routine activities, seek consultation with a qualified urologist for personalized evaluation and treatment.
Transobturator Tape (TOT) is a minimally invasive surgical procedure used to treat Stress Urinary Incontinence (SUI) in women — a condition where urine leaks involuntarily during activities that increase abdominal pressure such as coughing, sneezing, laughing, or exercising. TOT provides support to the urethra, restoring normal bladder control and improving quality of life.
The TOT procedure is designed to provide mid-urethral support by placing a synthetic mesh tape under the urethra. This tape acts like a sling, preventing urine leakage during physical strain. It offers a high success rate, shorter recovery time, and minimal postoperative discomfort compared to traditional surgeries.
TOT is typically recommended for women who have:
Stress Urinary Incontinence not responding to conservative measures like pelvic floor exercises.
Weak Pelvic Floor Muscles due to childbirth, menopause, or aging.
Recurrent SUI after previous treatments.
Normal bladder function but poor urethral support.
Before undergoing the TOT procedure, a detailed evaluation is essential to determine suitability and ensure optimal outcomes.
Preoperative Assessment May Include:
Medical History and Physical Examination: To assess symptoms, lifestyle factors, and overall health.
Urodynamic Testing: Measures bladder pressure and urine flow to confirm the type of incontinence.
Cystoscopy: Examines the bladder and urethra for abnormalities.
Urinalysis: To rule out urinary tract infections or other conditions.
The Transobturator Tape surgery is performed under local, regional, or general anesthesia and usually takes about 30–45 minutes.
Step-by-Step Overview:
A small incision is made in the vaginal wall beneath the urethra.
The synthetic mesh tape is inserted through the obturator foramen (a natural opening in the pelvic bone) on both sides of the pelvis.
The tape is positioned under the mid-urethra to act as a supportive sling.
The ends of the tape are adjusted to achieve proper tension — not too tight, to avoid urinary obstruction.
The incisions are closed, and no catheter is usually required beyond a few hours post-surgery.
The TOT technique offers several benefits compared to traditional methods of treating stress urinary incontinence.
Key Advantages Include:
Minimally invasive with smaller incisions
Shorter hospital stay and faster recovery
Reduced risk of bladder or bowel injury
Less postoperative pain
High success rate in restoring continence
Can often be performed as a day-care procedure
Most patients recover quickly after TOT surgery and can return to normal activities within a few days.
Post-Surgery Instructions:
Avoid heavy lifting or strenuous activities for 4–6 weeks.
Refrain from sexual intercourse until complete healing (typically 4 weeks).
Maintain good perineal hygiene.
Follow-up visits with your urologist to monitor recovery.
Report any signs of infection, pain, or difficulty urinating promptly.
While TOT is a safe and effective procedure, minor complications can occasionally occur.
Possible Risks Include:
Mild vaginal or groin discomfort
Temporary difficulty in urination
Urinary tract infection
Rarely, mesh exposure or erosion
Persistent or recurrent incontinence (in some cases)
Most complications, if they occur, are mild and can be managed effectively with prompt medical care.
TOT has shown excellent long-term success rates, with 80–90% of patients experiencing significant improvement or complete resolution of stress urinary incontinence symptoms. The procedure provides durable support and restores confidence in daily life activities.
Transobturator Tape (TOT) is a safe, minimally invasive, and highly effective surgical option for women suffering from Stress Urinary Incontinence. By providing reliable mid-urethral support, it helps restore urinary control and improves overall quality of life. If conservative measures have failed to relieve your symptoms, consult a qualified urologist or urogynecologist to determine if TOT is the right treatment for you.
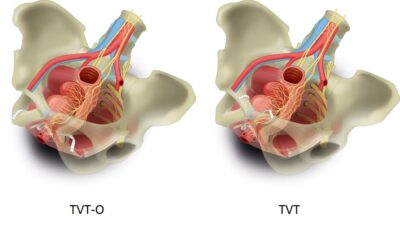
Tension-Free Vaginal Tape (TVT) is a minimally invasive surgical procedure used to treat Stress Urinary Incontinence (SUI) in women. SUI is a common condition characterized by involuntary leakage of urine during activities that increase abdominal pressure such as coughing, sneezing, laughing, or exercising. The TVT procedure provides effective, long-term relief by supporting the urethra and restoring normal urinary control.
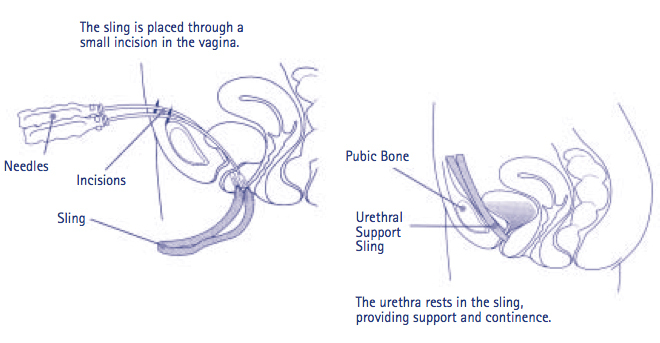
The TVT procedure is designed to create a supportive sling beneath the urethra using a narrow strip of synthetic mesh. This sling supports the urethra in its natural position, helping it remain closed during physical activity, thereby preventing urine leakage.
TVT is called “tension-free” because the tape is placed without applying pressure or tension on the urethra, reducing the risk of urinary obstruction and allowing the body to heal naturally around the tape for optimal support.
The TVT procedure is typically recommended for women who have:
Stress Urinary Incontinence not responsive to conservative treatments such as pelvic floor exercises.
Weak or damaged pelvic floor muscles due to childbirth, menopause, or aging.
Recurrent SUI after other surgical or non-surgical treatments.
Normal bladder function but poor urethral closure during strain.
Before undergoing the TVT procedure, a complete medical assessment is performed to confirm the diagnosis and determine the best surgical approach.
Preoperative Assessment May Include:
Detailed Medical History and Examination: To evaluate urinary symptoms and contributing factors.
Urinalysis: To rule out urinary tract infection.
Urodynamic Testing: To measure bladder and urethral function.
Cystoscopy: To inspect the bladder and urethra for abnormalities.
The Tension-Free Vaginal Tape (TVT) surgery is performed under local, regional, or general anesthesia and usually takes 30–45 minutes.
Step-by-Step Overview:
A small incision is made in the vaginal wall just beneath the urethra.
Two tiny incisions are made in the lower abdomen, near the pubic bone.
The synthetic mesh tape is inserted through these incisions and positioned under the mid-urethra to act as a supportive sling.
The tape is left “tension-free,” allowing the body’s tissues to secure it naturally.
The incisions are closed, and the patient is monitored for a few hours post-surgery.
Most patients are discharged on the same day or within 24 hours.
The TVT technique is one of the most widely performed and well-researched treatments for stress urinary incontinence, offering excellent long-term outcomes.
Key Advantages Include:
Minimally invasive with small incisions
Short hospital stay and quick recovery
High success and satisfaction rates
Minimal postoperative discomfort
Proven long-term safety and effectiveness
Recovery from TVT surgery is generally quick, and most patients resume normal activities within a few days.
Post-Surgery Instructions:
Avoid heavy lifting, exercise, and sexual activity for 4–6 weeks.
Maintain good perineal hygiene.
Follow prescribed medications and attend follow-up appointments.
Report any unusual pain, bleeding, or difficulty urinating promptly.
Although TVT is considered a safe and reliable procedure, minor complications can occasionally occur.
Possible Risks Include:
Temporary difficulty in urination
Urinary tract infection
Mild pelvic or abdominal discomfort
Mesh exposure or erosion (rare)
Persistent or recurrent incontinence in some cases
Early medical attention ensures timely management of any postoperative issues.
TVT has an excellent success rate, with studies showing 80–90% long-term improvement or cure in patients with stress urinary incontinence. The procedure provides durable urethral support, leading to restored confidence and improved quality of life.
Tension-Free Vaginal Tape (TVT) is a safe, effective, and minimally invasive surgical solution for women suffering from Stress Urinary Incontinence. By supporting the urethra without tension, TVT restores normal urinary control and significantly enhances quality of life. If you experience urine leakage during physical activity, consult a qualified urologist or urogynecologist to determine whether the TVT procedure is right for you.
Pubovaginal Sling (PVS) surgery is a well-established and effective treatment for Stress Urinary Incontinence (SUI) — a condition characterized by involuntary urine leakage during activities such as coughing, sneezing, laughing, or exercising. The PVS procedure restores normal urinary control by providing firm support to the urethra and bladder neck, helping prevent leakage during physical stress.
The Pubovaginal Sling procedure aims to provide long-term support to the urethra by using a strip of tissue or synthetic material as a sling. This sling acts like a hammock beneath the urethra, supporting it and helping maintain proper closure during increased abdominal pressure.
Unlike mid-urethral sling procedures such as TVT or TOT, the PVS sling is placed at the bladder neck, making it especially useful in patients with more severe or recurrent stress incontinence.
PVS surgery is recommended for women who have:
Moderate to severe Stress Urinary Incontinence
Intrinsic Sphincter Deficiency (ISD) — poor urethral closure due to weakened sphincter muscles
Recurrent SUI after failed mid-urethral sling or other procedures
Anatomical abnormalities or complex pelvic floor issues
History of pelvic surgeries that limit other surgical options
The sling material used in PVS may vary based on the patient’s condition and surgeon’s preference.
Common Sling Types Include:
Autologous Slings: Made from the patient’s own tissue (commonly rectus fascia from the lower abdomen).
Allograft Slings: Donor tissue from another human source.
Synthetic Slings: Made from biocompatible mesh materials.
Autologous slings are preferred in patients where synthetic mesh is contraindicated or in cases of previous mesh-related complications.
A thorough evaluation ensures that the PVS procedure is appropriate and safe for the patient.
Preoperative Assessment May Include:
Comprehensive Medical History and Physical Examination
Urinalysis and Urine Culture: To rule out infections.
Urodynamic Testing: Measures bladder and urethral function.
Cystoscopy: To inspect the bladder and urethra for abnormalities.
The Pubovaginal Sling surgery is performed under regional or general anesthesia and usually takes about 60–90 minutes.
Step-by-Step Overview:
A small incision is made in the vaginal wall beneath the urethra.
A strip of tissue (or synthetic mesh) is harvested and prepared if an autologous sling is used.
The sling is positioned under the bladder neck or urethra and its ends are passed behind the pubic bone.
The sling is secured to provide appropriate support without tension.
The incisions are closed, and a temporary catheter is placed to allow bladder drainage during initial healing.
The PVS procedure is a proven and durable solution, especially in complex or recurrent cases of stress urinary incontinence.
Key Advantages Include:
Long-term and durable results
Effective for severe or recurrent SUI
Suitable for patients with intrinsic sphincter deficiency
Can use the patient’s own tissue (autologous sling)
Low recurrence rate
Recovery after PVS surgery varies based on the type of sling used and the individual’s overall health.
Post-Surgery Instructions:
A urinary catheter may remain for 1–3 days post-surgery.
Avoid heavy lifting, bending, and strenuous activities for 4–6 weeks.
Maintain proper hygiene to prevent infection.
Follow up with your surgeon for regular evaluation and recovery monitoring.
Report any signs of infection, pain, or difficulty urinating promptly.
While the PVS procedure is generally safe, as with any surgery, some risks may occur.
Possible Risks Include:
Temporary difficulty in urination
Urinary tract infection
Vaginal discomfort or bleeding
Urinary retention (rarely requires sling adjustment)
Recurrent or persistent incontinence in some cases
Most patients recover well, and complications, if they occur, can be effectively managed with medical care.
The Pubovaginal Sling surgery has demonstrated long-term success rates of 85–90%, making it one of the most effective surgical treatments for stress urinary incontinence. The use of autologous tissue offers excellent biocompatibility and reduces the risk of rejection or erosion.
Pubovaginal Sling (PVS) is a reliable, time-tested, and effective surgical option for women suffering from Stress Urinary Incontinence, particularly those with recurrent or severe symptoms. By providing strong and lasting urethral support, PVS significantly improves urinary control, comfort, and quality of life. If you experience persistent urinary leakage or have not found relief from other treatments, consult a urologist or urogynecologist to determine if a Pubovaginal Sling is right for you.
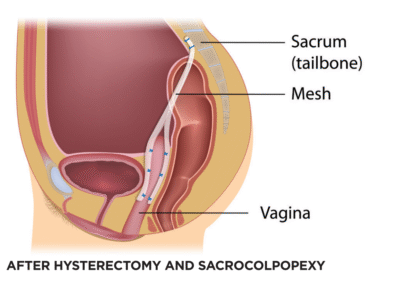
Robotic Sacrocolpopexy is a minimally invasive surgical procedure used to treat Pelvic Organ Prolapse (POP) — a condition in which the pelvic organs, such as the bladder, uterus, or vaginal vault, descend from their normal position and bulge into or outside the vaginal canal.
This advanced procedure uses robotic-assisted laparoscopic technology to restore normal pelvic anatomy by reattaching the vaginal vault or uterus to the sacrum (lower spine) using a surgical mesh. Robotic sacrocolpopexy offers high precision, less pain, minimal scarring, and faster recovery compared to traditional open surgery.
The goal of Robotic Sacrocolpopexy is to provide long-term support to the pelvic organs and relieve symptoms caused by pelvic organ prolapse, including pelvic pressure, vaginal bulge, urinary or bowel difficulties, and sexual discomfort.
The robotic platform allows the surgeon enhanced dexterity, 3D visualization, and fine control, making the procedure safer and more accurate.
This procedure is recommended for women with moderate to severe pelvic organ prolapse who wish to preserve vaginal function and achieve durable anatomical correction.
Common Indications Include:
Vaginal Vault Prolapse: Common after hysterectomy.
Uterine Prolapse: Descent of the uterus into the vaginal canal.
Cystocele: Bladder prolapse into the vagina.
Rectocele: Prolapse of the rectum into the vaginal wall.
Enterocele: Small bowel herniation into the vaginal apex.
A detailed assessment is crucial to ensure suitability for robotic sacrocolpopexy and to identify any underlying conditions that may need concurrent treatment.
Preoperative Evaluation May Include:
Comprehensive Pelvic Examination: To assess the degree and type of prolapse.
Urodynamic Testing: Evaluates bladder function and checks for urinary incontinence.
Pelvic Ultrasound or MRI: To visualize pelvic structures.
Medical History and Laboratory Tests: To ensure overall fitness for surgery.
Robotic Sacrocolpopexy is performed under general anesthesia and typically takes 2–3 hours. It uses small incisions in the abdomen through which robotic instruments and a camera are inserted.
Step-by-Step Overview:
Port Placement: Several small incisions are made for robotic arms and the camera.
Dissection: The surgeon separates the bladder, vagina, and rectum to prepare for mesh placement.
Mesh Placement: A Y-shaped surgical mesh is attached to the vaginal vault or cervix and then anchored to the sacrum (tailbone).
Securing the Mesh: The mesh supports the vagina or uterus, restoring its normal position.
Closure: The peritoneum (abdominal lining) is closed over the mesh to prevent bowel contact and minimize complications.
The robotic system allows delicate and precise movements, ensuring accurate placement and strong fixation of the mesh.
This robotic-assisted approach offers numerous benefits over traditional open or laparoscopic surgery.
Key Advantages Include:
Minimally invasive with small incisions
Shorter hospital stay and faster recovery
Reduced postoperative pain and blood loss
Minimal scarring and faster return to normal activities
Enhanced precision and durability of results
Excellent long-term anatomical and functional outcomes
Recovery from Robotic Sacrocolpopexy is generally smooth and quicker than conventional surgery.
Post-Surgery Instructions:
Most patients can return home within 24–48 hours.
Avoid heavy lifting, straining, or sexual activity for 6–8 weeks.
Maintain proper wound hygiene.
Follow up regularly with your surgeon to ensure proper healing.
Report symptoms such as fever, pain, or abnormal discharge immediately.
Although rare, certain risks can occur with any surgical procedure.
Possible Risks Include:
Infection or bleeding
Urinary tract infection
Mesh erosion or exposure (rare with modern materials)
Recurrence of prolapse (rare)
Injury to bladder, bowel, or blood vessels (very uncommon)
Most complications are minimal and manageable with prompt medical attention.
Robotic Sacrocolpopexy has one of the highest success rates among prolapse surgeries, with studies showing 85–95% long-term anatomical correction and high patient satisfaction. It restores pelvic support, relieves pressure symptoms, and maintains sexual and urinary function with minimal discomfort.
Robotic Sacrocolpopexy represents the gold standard in surgical management of Pelvic Organ Prolapse, offering superior precision, safety, and long-term results. This minimally invasive, robot-assisted technique restores normal pelvic anatomy, enhances comfort, and improves quality of life.
If you are experiencing symptoms of pelvic organ prolapse, consult a qualified urologist or urogynecologist to discuss whether robotic sacrocolpopexy is the right treatment option for you.
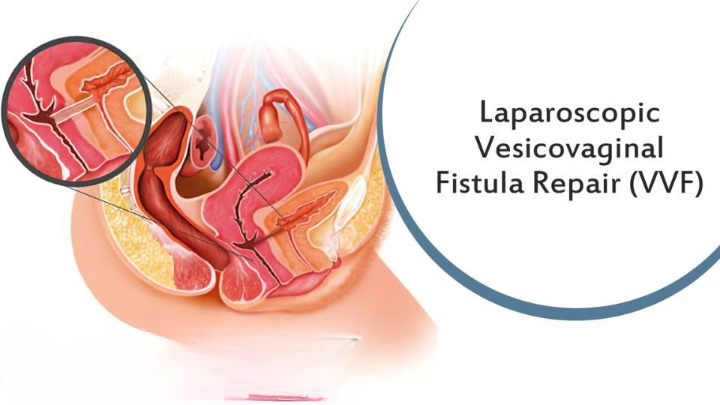
VVF commonly develops as a result of injury or trauma to the bladder or vaginal wall. The main causes include:
Surgical Trauma: The most frequent cause, often following gynecological surgeries such as hysterectomy.
Obstetric Complications: Prolonged or obstructed labor can cause tissue necrosis leading to fistula formation.
Radiation Therapy: Pelvic radiation for cancer treatment may damage bladder tissues.
Pelvic Malignancies: Advanced cervical or bladder cancers can erode into adjacent organs.
Infection or Injury: Rarely, infections or accidental trauma can result in VVF.
The hallmark symptom of VVF is continuous urinary leakage through the vagina, regardless of urination. Other symptoms may include:
Constant wetness and irritation in the vaginal area
Foul-smelling vaginal discharge
Recurrent urinary tract infections (UTIs)
Discomfort during sexual intercourse (dyspareunia)
Emotional distress and social embarrassment due to incontinence
A proper diagnosis is essential for effective treatment planning. Your urologist or urogynecologist will perform a thorough evaluation which may include:
Medical History and Physical Examination: To assess symptoms, prior surgeries, or obstetric history.
Dye Test (Methylene Blue Test): A simple in-office test used to confirm urinary leakage from the bladder to the vagina.
Cystoscopy: Direct visualization of the bladder and fistula tract to determine its location and size.
Imaging Tests: Ultrasound, CT Urography, or MRI may be used for detailed assessment and surgical planning.
The treatment approach depends on the size, location, cause, and duration of the fistula, as well as the patient’s overall health. Surgery remains the mainstay of management.
In very small and recent fistulas, continuous bladder drainage with a catheter for several weeks may allow spontaneous closure. However, this approach is rarely sufficient for established cases.
Surgical closure is the definitive treatment for vesicovaginal fistula. The procedure can be performed through different approaches:
Transvaginal Approach: Preferred for low and small fistulas; involves accessing and closing the fistula through the vagina.
Transabdominal Approach: Used for high or complex fistulas; allows better visualization of the bladder and ureters.
Laparoscopic or Robotic Repair: Minimally invasive techniques offering faster recovery, minimal pain, and reduced hospital stay.
During the procedure, the fistula is carefully dissected, the edges are refreshed, and the bladder and vaginal walls are closed separately in multiple layers to ensure watertight healing. Sometimes, tissue flaps (like the Martius flap or omental flap) are used to strengthen the repair and improve healing.
Post-surgery care is crucial for optimal healing and successful outcomes:
Continuous bladder drainage with a Foley catheter for 2–3 weeks
Antibiotic therapy to prevent infections
Avoiding sexual intercourse and heavy activity until complete healing
Regular follow-up visits and imaging if needed
With experienced surgical care, VVF repair has a high success rate (over 90%). Most women regain full bladder control and quality of life. Early detection, proper surgical technique, and good postoperative care are key factors in ensuring a successful recovery.
VVF Repair is a life-restoring procedure that addresses one of the most distressing urological complications affecting women. With timely diagnosis and expert surgical management, patients can achieve complete continence, improved confidence, and a return to normal life. If you experience persistent urinary leakage or symptoms suggestive of a fistula, consult a urologist promptly for evaluation and treatment.
Dr. Rohit Kaushal is a leading Urologist and Robotic Surgeon in Delhi, specializing in kidney transplant, prostate, and reconstructive urology with compassionate patient care.
© 2025 Created with Digital Growth Well