Andrology is the dedicated field focusing on male health, specifically related to the male reproductive and urinary systems. We offer comprehensive diagnostic and advanced therapeutic solutions for male infertility, hormonal imbalances (such as low testosterone), and sexual health issues. Our approach combines meticulous clinical evaluation with cutting-edge treatments to help men achieve optimal reproductive health and fulfill their family goals.

Erectile Dysfunction (ED) is a common condition affecting millions of men worldwide. Defined as the persistent inability to achieve or maintain an erection sufficient for satisfactory sexual performance, ED can significantly impact emotional well-being, relationships, and overall quality of life. Understanding its causes and undergoing a proper clinical evaluation are essential for effective management and successful treatment.
ED is often multifactorial, stemming from physical, psychological, or lifestyle-related issues:
Cardiovascular Issues: Conditions like atherosclerosis (hardening of the arteries) can reduce blood flow to the penis, a primary cause of ED.
Diabetes: High blood sugar can damage the blood vessels and nerves necessary for an erection.
Hormonal Imbalances: Low testosterone levels can lead to diminished libido and ED. Thyroid function tests may also be relevant.
Neurological Disorders: Conditions such as Parkinson’s disease or multiple sclerosis can affect the nerve signals from the brain to the penis.
Chronic Illnesses: Conditions like hypertension (high blood pressure) and kidney disease are frequently contributing factors.
Stress and Anxiety: Performance anxiety or general life stress can profoundly affect sexual function.
Depression: This mental health issue often leads to decreased libido and erectile problems.
Relationship Issues: Conflict, communication problems, or other relational stress can contribute to ED.
Smoking and Alcohol Use: Both can impair blood flow and nerve function.
Obesity: Excess weight can lead to hormonal changes and vascular problems.
Sedentary Lifestyle: A lack of physical activity contributes to overall poor cardiovascular health.
A comprehensive evaluation is crucial for accurately diagnosing ED and identifying its underlying causes. Here is what to expect during a clinical assessment with a urologist:
The urologist will take a detailed history, covering:
Symptoms: Duration and severity of the issue and its impact on life.
Medical Conditions: Any existing health issues (e.g., diabetes, heart disease, hormone disorders).
Medications: Reviewing current prescriptions, as certain drugs can contribute to ED.
Psychosocial Factors: Evaluating stressors, mental health status, and relationship dynamics.
A thorough physical exam helps identify signs of underlying health conditions:
Genital Examination: Checking for any physical abnormalities in the genitalia.
Cardiovascular Assessment: Evaluating blood pressure and heart health.
Neurological Assessment: Testing reflexes and sensory responses.
Depending on the initial evaluation, necessary tests may include:
Blood Tests: To check testosterone levels, blood sugar (glucose), cholesterol, and thyroid function.
Urinalysis: To assess for diabetes or other metabolic issues.
In some cases, additional diagnostic testing is recommended:
Penile Doppler Ultrasound: An imaging test to precisely evaluate blood flow to and from the penis.
Office Sildenafil Test: A diagnostic test involving the administration of an ED medication under supervision.
Nocturnal Penile Tumescence (NPT) Testing: Monitors erections during sleep to help differentiate between physical and psychological causes.
Penile Biothesiometry: Measures sensitivity in the penis, aiding in the assessment of nerve function.
Psychological Evaluation: If psychological factors are strongly suspected, a mental health assessment may be necessary to evaluate stress, anxiety, or depression.
Erectile dysfunction is a multifaceted condition that requires a thoughtful and thorough clinical evaluation. Early and accurate diagnosis, followed by a tailored treatment plan, can significantly improve sexual health and overall quality of life. If you or someone you know is experiencing symptoms of ED, seeking medical advice from a specialist is a vital first step toward addressing the issue. With proper evaluation and personalized treatment options, many men can successfully regain their sexual confidence and well-being.
Erectile Dysfunction (ED) is a widespread condition, impacting millions of men globally. Characterized by the consistent inability to achieve or maintain an erection firm enough for satisfactory sexual performance, ED can stem from both psychological and physical factors. Understanding the diverse medical management options available is key for those affected to reclaim their sexual health and overall well-being.
ED can arise from a complex interplay of various factors:
Psychological Causes: Stress, anxiety (including performance anxiety), depression, and relationship issues can significantly contribute to ED.
Physical Causes: Underlying health conditions such as diabetes, hypertension (high blood pressure), heart disease, and hormonal imbalances (e.g., low testosterone) can impede erectile function.
Lifestyle Factors: Habits like smoking, excessive alcohol consumption, obesity, and a sedentary lifestyle can also play a significant role in its development.
The effective treatment of ED typically begins with a thorough assessment by a healthcare provider, including a detailed medical history and physical examination. Depending on the identified underlying causes, several medical management options may be considered.
The most common first-line treatment for ED is oral phosphodiesterase type 5 (PDE5) inhibitors. These medications work by enhancing blood flow to the penis and are highly effective for many men. Widely prescribed PDE5 inhibitors include:
Sildenafil (Viagra): Typically taken 30 minutes to an hour before sexual activity, with effects lasting up to four hours.
Tadalafil (Cialis): Known for its longer duration of action (up to 36 hours), Tadalafil can be taken daily or as needed, offering greater spontaneity.
Vardenafil (Levitra): Similar to Sildenafil, it also works quickly but may have a different side effect profile for some individuals.
Avanafil (Stendra): A newer option, it often works faster than others, with effects beginning in about 15 minutes.
It is crucial to note that these medications may not be suitable for everyone, particularly those with certain health conditions or who are taking specific medications (e.g., nitrates).
For men with ED related to hormonal deficiencies, such as low testosterone levels, hormone replacement therapy (HRT) may be recommended. This can involve:
Testosterone Replacement Therapy: Administered via injections, patches, gels, or pellets, this therapy can improve libido, energy levels, and overall sexual function, particularly when low testosterone is the primary cause.
VEDs are non-invasive mechanical devices that create a vacuum around the penis, drawing blood into the erectile tissues. Once an erection is achieved, a constriction ring is placed at the base of the penis to maintain the erection. This method can be effective for men who prefer not to take medications or for those who cannot use them due to health reasons.
For some men, direct administration of medication may be more effective:
Intracavernosal Injections: Medications such as alprostadil, bimix, or trimix can be injected directly into the penis, often leading to an erection within minutes.
Urethral Suppositories: Alprostadil is also available in a suppository form (MUSETM) that is inserted into the urethra.
These methods can be effective but require a certain level of training and comfort with self-administration.
For men who do not respond to other treatments or who prefer a more permanent solution, penile implants may be an option. Surgical procedures can place inflatable or malleable rods within the penis, allowing for controlled erections. This option typically has high satisfaction rates but involves surgery and a recovery period.
Beyond medical interventions, a holistic approach often includes:
Since psychological factors frequently play a significant role in ED, addressing these issues through therapy can be highly beneficial. Cognitive-behavioral therapy (CBT) or counseling can help men and their partners deal with the emotional aspects of ED, reducing anxiety and improving intimacy.
In addition to medical treatments, adopting healthy lifestyle changes can significantly enhance erectile function:
Quitting Smoking: Improves blood flow and overall cardiovascular health.
Limiting Alcohol: Moderation can help prevent erectile issues.
Exercising Regularly: Physical activity improves cardiovascular health, enhancing blood circulation.
Healthy Diet: A balanced diet can improve overall health and mitigate some physical causes of ED.
Erectile dysfunction can be a challenging condition, but a comprehensive range of effective medical management options exists. From oral medications and hormonal therapies to mechanical devices and surgical interventions, understanding these choices empowers men to seek appropriate help and improve their sexual health. Consulting with your urologist is crucial to determine the most appropriate treatment plan based on individual needs and underlying causes. With the right approach, many men can regain confidence and enjoy satisfying sexual relationships once again.
Erectile dysfunction (ED) affects millions of men worldwide, significantly impacting relationships and overall quality of life. While various treatment options exist, intracavernosal injection (ICI) therapy has emerged as a highly effective and reliable alternative, particularly for those seeking immediate and consistent results.
Intracavernosal injection therapy involves the direct administration of a specialized medication into the corpora cavernosa, the two spongy erectile tissues located along the sides of the penis. This method facilitates the rapid relaxation of blood vessels within these tissues, dramatically enhancing blood flow and thereby allowing for a firm, sustained erection in response to or even without sexual stimulation.
The primary medications used in ICI therapy, often in combination (e.g., “Trimix” or “Bimix”), work synergistically to induce an erection. These include:
Alprostadil: A synthetic form of prostaglandin E1 that powerfully dilates blood vessels, promoting increased blood flow into the penis.
Papaverine: An alkaloid that relaxes smooth muscles in the penile arteries, allowing them to expand.
Phentolamine: An alpha-adrenergic antagonist that further helps improve blood flow by blocking certain vasoconstricting receptors.
Chlorpromazine: Sometimes used in combination for its vasodilatory effects.
These medications typically induce an erection within 5 to 10 minutes after injection, making it a very rapid-acting treatment.
ICI therapy offers several significant advantages for men with ED:
High Efficacy: ICI therapy boasts a high success rate, typically ranging from 70-90%, making it one of the most effective treatments for ED. It is particularly valuable for men who do not respond to oral medications like sildenafil (Viagra), experience intolerable side effects from them, or have contraindications to their use.
Rapid Onset: Unlike oral medications that may take longer to take effect, ICI provides quicker results, which can be particularly advantageous for spontaneous sexual encounters.
Customizable Dosage: A urologist can precisely tailor the dosage based on an individual’s specific response, allowing for personalized and optimized treatment.
Alternative for Specific Conditions: ICI is often recommended for men with specific medical conditions (such as severe diabetes, post-prostatectomy ED, or nerve damage) that may render other treatments less effective.
While ICI therapy is generally safe and well-tolerated, it is essential to be aware of potential side effects and discuss them with your urologist:
Pain at Injection Site: Some men may experience mild discomfort, bruising, or a small hematoma at the injection site.
Priapism: A prolonged erection lasting more than four hours can occur. This is a medical emergency and necessitates immediate medical attention to prevent potential penile tissue damage.
Fibrosis: Repeated injections over a long period may lead to the formation of scar tissue (fibrosis) in the penis, which could potentially affect future erections or cause penile curvature.
Changes in Sensation: Some users report temporary changes in penile sensitivity or an altered sensation during ejaculation.
Before initiating ICI therapy, a thorough medical evaluation is necessary. Key points to consider include:
Consultation with a Specialist: A qualified urologist will assess the underlying causes of ED and determine if ICI therapy is the appropriate treatment for your specific needs.
Proper Injection Technique: Patients must receive comprehensive training on how to self-administer the injections safely and effectively to minimize risks and ensure optimal results.
Regular Monitoring: Follow-up appointments are crucial to monitor efficacy, identify any side effects, and make necessary adjustments to the dosage.
Intracavernosal injection therapy offers a robust and highly effective solution for men struggling with erectile dysfunction, especially those who have not found relief through other treatments. Its high efficacy and rapid action make it an attractive option, though potential side effects and the importance of proper technique and medical supervision should not be overlooked. If you are considering ICI therapy, consult with your urologist to discuss whether it is the right choice for your individual needs. With the right approach and guidance, many men can successfully regain confidence and significantly improve their sexual health and well-being.
Penile implants are advanced medical devices designed to effectively treat Erectile Dysfunction (ED), particularly when other therapeutic options have proven unsuccessful. Significant advancements in medical technology have led to a variety of implant types, each offering distinct benefits and considerations. Careful patient selection is paramount to ensuring successful outcomes and high patient satisfaction following surgery.
There are primarily two main types of penile implants available:
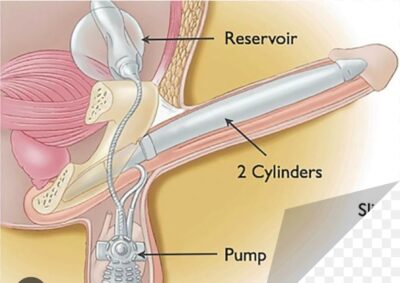
Inflatable implants are the most commonly used type today, offering a discreet and natural-looking solution. They consist of:
Two Cylinders: Surgically placed within the penis.
A Reservoir: Placed discreetly in the lower abdomen.
A Pump: Located within the scrotum.
How They Work: When the patient wishes to achieve an erection, they activate the pump, which transfers fluid from the reservoir to the cylinders, causing them to inflate and firm the penis. Advantages: These implants provide a natural-looking and feeling erection, and can be deflated after intercourse, allowing for a more spontaneous experience and excellent concealment. Disadvantages: The mechanical complexity of the device may lead to a risk of mechanical failure in some rare cases.
Malleable implants consist of two bendable rods that are surgically inserted into the penis.
How They Work: The rods provide constant rigidity, allowing the penis to be manually adjusted to an upright position for intercourse and bent down against the body when not in use. Advantages: Simplicity and high reliability are key benefits, as they have fewer mechanical parts and a lower risk of mechanical failure compared to inflatable implants. Disadvantages: The penis is always in a semi-rigid state, which may be less desirable for some patients regarding its concealment.
Choosing the appropriate candidates for penile implant surgery is critical for maximizing success rates and patient satisfaction. Here are some key factors considered during evaluation:
Underlying Health Conditions: Patients with a history of severe cardiovascular disease, uncontrolled diabetes, or other significant comorbidities may be at higher risk for complications. A thorough medical evaluation is essential to assess surgical fitness.
Psychological Evaluation: ED often has significant psychological components, such as anxiety or depression. Assessing a patient’s mental health and ensuring they have realistic expectations about the surgery’s outcomes is vital for overall satisfaction.
Failure of Other Treatments: Ideal candidates should have conscientiously tried and failed other non-surgical ED treatments, such as oral medications (PDE5 inhibitors), injections, or vacuum erection devices. This step confirms the necessity and suitability for an implant.
Desire for Sexual Function Restoration: The patient must express a strong and clear desire to restore sexual function. Transparent communication about the potential risks, benefits, and limitations of surgery is essential.
Age and Lifestyle Factors: Younger patients may have different expectations and needs compared to older patients. Additionally, lifestyle factors such as smoking, substance abuse, or poor physical health can affect outcomes and should be addressed prior to surgery.
Surgeon Experience and Technique: The choice of a urologist highly experienced in penile implant surgery can significantly influence the outcome. Surgeons should discuss their approach, success rates, and potential complications transparently with the patient.
Penile implants can dramatically improve the quality of life for men suffering from severe or refractory ED. Understanding the different types of implants and meticulously selecting the right patients are essential steps in the treatment process. By carefully considering medical history, psychological factors, and patient expectations, your urologist can guide patients toward a treatment plan that best meets their individual needs. Ultimately, the goal is to enhance sexual function, restore confidence, and lead to a more fulfilling life.
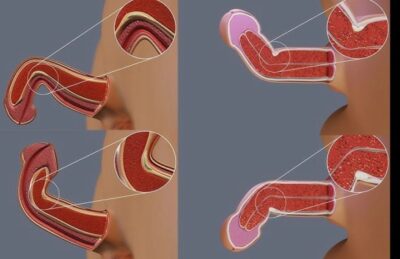
Peyronie’s disease is a connective tissue disorder affecting the penis, characterized by the formation of fibrous scar tissue (plaques) beneath the skin. This condition can lead to painful erections, significant penile curvature, and difficulties with sexual function, including erectile dysfunction, profoundly impacting a man’s quality of life.
The exact cause of Peyronie’s disease remains unclear, but several factors are believed to contribute:
Trauma or Injury: Physical injury to the penis, often during sexual activity or other incidents, can trigger the development of scar tissue.
Genetic Factors: A family history of Peyronie’s disease or similar connective tissue disorders may increase the risk.
Connective Tissue Disorders: Conditions such as Dupuytren’s contracture, which affects the hands, may be linked to Peyronie’s disease.
Age: The risk of developing Peyronie’s disease tends to increase with age.
Comorbidities: Conditions like diabetes may be associated with an increased risk of developing Peyronie’s disease.
Symptoms of Peyronie’s disease typically include:
Curvature of the penis during erection.
Pain during erections or when touching the penis.
Difficulty achieving or maintaining an erection (erectile dysfunction).
A noticeable lump or hardened area (plaque) on the shaft of the penis.
Shortening or narrowing of the penis.
The diagnosis of Peyronie’s disease usually involves a comprehensive evaluation:
Medical History: A thorough discussion of symptoms, sexual history, and any potential penile injuries.
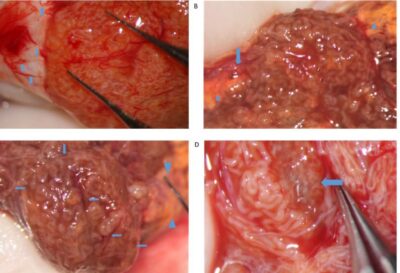
Physical Examination: A healthcare provider will carefully examine the penis for curvature, lumps, or plaques.
Imaging Tests: In some cases, a penile ultrasound may be used to assess the plaques, measure their size, and evaluate blood flow to the penis, especially if there are concerns about coexisting erectile dysfunction.
Penile Mapping: This is a more detailed assessment that often involves inducing an erection (pharmacologically) to accurately determine the extent and degree of the curvature and plaque location.
Treatment for Peyronie’s disease varies based on the severity of the condition, its impact on the patient’s sexual function, and whether the disease is in its acute (inflammatory) or chronic (stable) phase. Here are some common approaches:
Observation: In mild cases where symptoms do not significantly affect sexual function, or during the early, active phase of the disease, a watch-and-wait approach may be recommended, as some symptoms can improve over time.
Medications: Oral Medications: While no single oral medication is universally FDA-approved specifically for Peyronie’s, some drugs like Vitamin E, Pentoxifylline, and Potaba have been used with varying degrees of success in reducing plaque size or curvature, especially in the early stages.
Injectable Medications: Options like collagenase Clostridium histolyticum (Xiaflex) can be injected directly into the plaque to help break down the collagen, potentially reducing curvature and improving penile deformity.
Vacuum Devices: Involves using a vacuum erection device (VED) to help stretch the penile tissues, potentially reducing curvature and improving erectile function.
Penile Traction Therapy: Various types of penile traction devices are now available which, when used consistently, can prevent penile shortening and may lead to slight lengthening of the penis, particularly in the active phase of the disease.
Surgery: For severe cases, when conservative treatments fail, or once the disease has stabilized (typically for 3-6 months with no change in curvature), surgical options may be considered:
Plication Surgery: This involves shortening the side of the penis opposite the plaque to straighten it, suitable for less severe curvatures with good erectile function.
Grafting: If the curvature is significant or there is significant shortening, a graft can be placed over the area of the plaque to help restore the penis’s straightness and potentially length.
Penile Implants: In cases where severe erectile dysfunction is also present and unresponsive to other treatments, penile implants may be placed to provide rigidity and help straighten the penis.
Shockwave Therapy (ESWT): Emerging treatments like low-intensity extracorporeal shockwave therapy are being studied for their potential to reduce pain and improve penile curvature, particularly in the early stages.
Peyronie’s disease can be a distressing condition, but it’s essential to know that effective diagnosis and a range of tailored treatment options are available. If you suspect you have Peyronie’s disease or are experiencing related symptoms, it’s crucial to consult your urologist promptly. Early intervention can often lead to better outcomes, allowing you to regain confidence, improve sexual function, and enhance your overall quality of life.
Priapism is a medical emergency condition characterized by a prolonged and often painful erection that occurs without sexual arousal or stimulation. This condition can pose serious health risks and requires prompt attention.
Priapism is generally classified into two main types:
This type is less common and typically less painful. Non-ischemic priapism occurs when there is an abnormal connection between the arteries and veins, often resulting from blunt trauma. Blood flows freely into the penis, which can lead to prolonged erections without the severe pain associated with ischemic priapism.
Arterial Injury: Penile or pelvic trauma can lead to non-ischemic priapism.
Spontaneous Causes: Rarely, it can occur without any identifiable cause.
Diagnosis begins with a thorough medical history and physical examination. Your urologist will assess the duration, pain level, and possible triggers of the erection. Diagnostic tools may include:
Blood Tests: To check for sickle cell disease or other blood disorders.
Doppler Ultrasound: This imaging test can evaluate blood flow in the penis, helping differentiate between ischemic and non-ischemic priapism.
Penile Blood Gas Analysis: A more invasive test, this involves drawing blood from the penis to assess oxygen and carbon dioxide levels, which helps in diagnosing ischemic priapism.
The treatment for priapism varies based on the type and underlying cause.
Ice Packs: Applying cold compresses can help reduce blood flow and swelling.
Medications: Intracavernosal injections of sympathomimetic agents (e.g., epinephrine or phenylephrine) can help constrict blood vessels and relieve the erection.
Aspiration: Your urologist may use a needle and syringe to withdraw excess blood from the penis.
Surgery: If other treatments fail, surgical options may include creating a shunt to divert blood flow.
Treatment for non-ischemic priapism is typically less aggressive, as it is often self-limiting. Options include:
Observation: Many cases resolve spontaneously.
Arterial Embolization: A minimally invasive procedure to block blood flow to the affected area if symptoms persist.
Priapism is considered a medical emergency if an erection lasts longer than four hours, especially in cases of ischemic priapism. Prolonged ischemic priapism can lead to permanent erectile dysfunction and other complications.
Priapism, while uncommon, can have significant implications for men’s health. Understanding its types, causes, and treatment options is crucial for effective management. If you or someone you know experiences prolonged or painful erections, seeking medical attention promptly is essential to prevent serious complications.
Sexually transmitted infections (STIs) are a significant public health concern worldwide. With millions of new cases diagnosed each year, understanding STIs, their prevention, and their treatment is crucial for maintaining sexual health.
STIs are infections that are primarily spread through sexual contact, including vaginal, anal, and oral sex. They can be caused by various pathogens, including bacteria, viruses, and parasites. Common STIs include:
Chlamydia
Gonorrhea
Syphilis
HIV/AIDS
Herpes Simplex Virus (HSV)
Human Papillomavirus (HPV)
Trichomoniasis
Many STIs can be asymptomatic, meaning individuals may not experience noticeable symptoms. However, when symptoms do occur, they can include:
Unusual discharge from the genitals
Pain during urination
Sores or bumps in the genital area
Flu-like symptoms (in the case of HIV)
Untreated STIs can lead to severe health complications, including infertility, chronic pain, and an increased risk of contracting or transmitting HIV.
Preventing STIs is key to promoting sexual health. Here are some effective strategies:
Use Condoms: Consistent and correct use of condoms significantly reduces the risk of many STIs.
Regular Testing: Routine STI screenings can help identify infections early, even when no symptoms are present.
Limit Sexual Partners: Reducing the number of sexual partners can lower the risk of exposure to STIs.
Vaccination: Vaccines are available for certain STIs, including HPV and hepatitis B, which can help prevent infection.
Open Communication: Discussing sexual health and STI testing with partners can promote safer sexual practices.
Most bacterial STIs can be effectively treated with antibiotics. Viral STIs, like HIV and herpes, cannot be cured but can be managed with antiviral medications. Early diagnosis and treatment are crucial to prevent complications and reduce transmission.
Despite being common, STIs carry a stigma that can prevent individuals from seeking testing and treatment. It’s essential to foster an open dialogue about sexual health, emphasizing that STIs can affect anyone, regardless of age, gender, or sexual orientation.
Sexually transmitted infections are a critical aspect of public health that requires awareness, prevention, and proactive management. By prioritizing sexual health through education, communication, and regular testing, individuals can reduce their risk and contribute to healthier communities.
Remember, your sexual health is just as important as any other aspect of your well-being. Don’t hesitate to reach out to healthcare professionals for guidance and support.

Circumcision has been performed for centuries for various cultural, religious, and medical reasons. Recently, a method known as stapler circumcision has emerged as a popular technique due to its efficiency and minimally invasive nature.
Stapler circumcision is a surgical technique that utilizes a specialized stapling device to remove the distal foreskin from the penis. This method is often performed under local anaesthesia. The stapler device is designed to ensure precise cuts, minimizing tissue damage and reducing recovery time.
The procedure involves the following steps:
1. Preparation: The patient is positioned comfortably, and the area is sterilized.
2. Anaesthesia: Local anesthesia is administered to numb the area.
3. Stapler Application: The stapler device is positioned around the foreskin. Once activated, it simultaneously cuts and staples the foreskin, allowing for controlled removal.
4. Post-Procedure Care: After the removal, the area is cleaned and dressed. Patients are given instructions for aftercare to promote healing and prevent infection.
1. Minimally Invasive: The stapler method is less invasive than traditional circumcision, leading to less blood loss and a lower risk of complications.
2. Reduced Recovery Time: Many patients experience quicker recovery times compared to traditional methods, often returning to normal activities within a few days.
3. Precision: The stapler allows for precise cuts, which can enhance cosmetic outcomes and reduce the likelihood of complications such as uneven skin removal.
4. Shorter Procedure Time: The stapler technique generally takes less time to perform than traditional surgical methods, making it more efficient for both patients and urologist.
While stapler circumcision offers several advantages, it’s essential to consider potential risks:
Infection: As with any surgical procedure, there is a risk of infection at the site.
Scarring: Improper technique or healing can lead to noticeable scarring.
Complications: Rarely, complications such as bleeding or necrosis may occur.
Before undergoing the procedure, it’s vital to discuss any concerns with your urologist. They can provide guidance on whether stapler circumcision is suitable based on individual health factors.
Stapler circumcision can be performed on individuals of various ages, including adolescents, and adults. It is often recommended for:
Cultural or Religious Reasons: Many families opt for circumcision for cultural or religious beliefs.
Medical Conditions: Conditions such as phimosis (tight foreskin) or recurrent infections may warrant the procedure.
Stapler circumcision is a modern, efficient approach to the traditional circumcision process, offering numerous benefits for patients seeking this option. Understanding the procedure, its advantages, and potential risks can help individuals make the best choice for their health and well-being.

A varicocele is a common male health condition defined as an abnormal enlargement of the veins (the pampiniform plexus) inside the scrotum, similar to varicose veins in the legs. As the most common surgically correctable cause of male infertility, a varicocele may also cause pain or progressive testicular damage.
Microsurgical Varicocelectomy is the preferred and most advanced surgical technique for correcting varicoceles, offering the highest success rates and lowest complication rates.
The enlarged veins impair testicular function primarily by:
Elevating Testicular Temperature: The pooled blood acts as an insulator, hindering the cooling mechanism required for healthy sperm production.
Impairing Spermatogenesis: The resulting poor blood flow can lead to low sperm count, poor sperm motility, and reduced sperm quality.
Testicular Atrophy: In adolescents and sometimes adults, the condition can cause the testicle to shrink.
Pain: Varicoceles can cause a dull ache or discomfort, especially with prolonged standing or physical activity.
The procedure is considered the gold standard due to its utilization of a high-powered operating microscope. This magnification is critical for precision:
Preservation of Vital Structures: The microscope allows the surgeon to meticulously identify and preserve the tiny testicular artery (essential for blood flow to the testicle) and the lymphatic vessels (essential for fluid drainage).
Complete Vein Ligation: It ensures that virtually all of the abnormal veins are identified and tied off (ligated), including the smaller veins often missed by non-microsurgical techniques.
Low Recurrence and Complication Rates: The high degree of precision results in significantly lower rates of varicocele recurrence and complications like hydrocele formation (fluid build-up around the testicle).
Microsurgical varicocelectomy is typically recommended for men with a palpable varicocele who present with one or more of the following:
Male Infertility: An abnormal semen analysis (low count, poor motility, or poor morphology) in a couple trying to conceive, where the female partner has normal or treatable fertility.
Testicular Pain: Chronic or persistent scrotal pain clearly attributed to the varicocele.
Testicular Atrophy: Shrinkage of the testicle, particularly in adolescents.
For men and couples dealing with varicocele-related infertility or discomfort, microsurgical varicocelectomy represents the most reliable and effective treatment option. Consulting with a specialist in male reproductive medicine and microsurgery is essential to discuss the procedure and its potential for a positive outcome.
varicocele is a common male health condition defined as an abnormal enlargement of the veins (the pampiniform plexus) inside the scrotum, similar to varicose veins in the legs. As the most common surgically correctable cause of male infertility, a varicocele may also cause pain or progressive testicular damage.
Microsurgical Varicocelectomy is the preferred and most advanced surgical technique for correcting varicoceles, offering the highest success rates and lowest complication rates. It is recognized as the gold-standard approach for varicocele repair in both adults and adolescents.
The enlarged veins impair testicular function primarily by:
Elevating Testicular Temperature: The pooled blood acts as an insulator, preventing the required cooling mechanism for healthy sperm production.
Impairing Spermatogenesis: The resulting poor blood flow can lead to low sperm count, poor sperm motility, and reduced sperm quality.
Testicular Atrophy: In adolescents and sometimes adults, the condition can cause the testicle to shrink.
Pain: Varicoceles can cause a dull ache or discomfort, especially with prolonged standing or physical activity.
The procedure is considered the gold standard due to its utilization of a high-powered operating microscope. This magnification is critical for precision:
Preservation of Vital Structures: The microscope allows the surgeon to meticulously identify and preserve the tiny testicular artery (essential for blood flow to the testicle) and the lymphatic vessels (essential for fluid drainage).
Complete Vein Ligation: It ensures that virtually all of the abnormal veins are identified and tied off (ligated), including the smaller veins often missed by non-microsurgical techniques.
Low Recurrence and Complication Rates: The high degree of precision results in significantly lower rates of varicocele recurrence (typically 1-2%) and complications like hydrocele formation (fluid build-up around the testicle, typically 0-1%).
Microsurgical varicocelectomy is typically recommended for men with a palpable varicocele who present with one or more of the following:
Male Infertility: An abnormal semen analysis (low count, poor motility, or poor morphology) in a couple trying to conceive, in the setting of normal or correctable female infertility.
Testicular Pain: Chronic or persistent scrotal pain clearly attributed to the varicocele.
Testicular Atrophy: Shrinkage of the testicle, particularly in adolescents.
Microsurgical varicocelectomy has proven to be highly effective with the following typical results:
Improved Fertility: Significant improvement in semen analysis parameters is seen in 60-80% of men. Pregnancy rates following the procedure often range from 40-70% when female factors are excluded or treated.
Pain Relief: Resolution of chronic varicocele-related pain is reported in 80-90% of men.
Hormone Improvement: The procedure can result in substantial improvement in serum testosterone levels in men with low levels prior to surgery.
Reversal of Atrophy: Catch-up growth of the testicle in adolescents.
For men and couples dealing with varicocele-related infertility, pain, or testicular atrophy, microsurgical varicocelectomy represents the most reliable and effective treatment option. Understanding its precision, high success rates, and low complication profile is crucial. Consulting with a specialist in male reproductive medicine and microsurgery is essential to determine the best course of action.
Male infertility refers to a male’s inability to cause pregnancy in a fertile female after one year of regular, unprotected sexual intercourse. It is a common issue, with male factors solely responsible for about 20% of all infertility cases and a contributing factor in an additional 30-40%.
The inability to conceive is often related to problems with the production, function, or delivery of sperm.
The causes of male infertility are diverse and can include:
Varicocele: Swelling of the veins that drain the testicle. This is the most common reversible cause and can lead to reduced sperm quantity and quality, possibly due to abnormal blood flow and temperature regulation.
Sperm Production or Function Issues:
Low or No Sperm Count (Oligospermia or Azoospermia): The semen contains too few sperm or none at all.
Abnormal Sperm Shape (Morphology) or Movement (Motility): Sperm that are malformed or unable to swim properly cannot fertilize an egg effectively.
Obstruction or Ejaculation Issues:
Infections: Infections (e.g., epididymitis, orchitis, or certain STIs) can interfere with sperm production or cause scarring that blocks sperm passage.
Ejaculation problems: Such as retrograde ejaculation, where semen enters the bladder instead of emerging from the penis.
Blockages: Defects or injuries in the tubes that transport sperm (like the vas deferens) can block the sperm’s passage.
Hormone Imbalances: Problems with the testicles, pituitary gland, hypothalamus, or other hormonal systems can disrupt sperm production.
Genetic or Chromosome Defects: Inherited disorders, such as Klinefelter’s syndrome, can affect the development of the reproductive organs.
Other Factors and Lifestyle:
Prior Surgery: Procedures like vasectomy, or surgeries for testicular/rectal cancer.
Medications: Certain drugs, including long-term anabolic steroid use, testosterone replacement therapy, and some cancer, ulcer, or arthritis medications.
Environmental/Lifestyle: Exposure to high heat, smoking, heavy alcohol or drug use, and obesity.
Undescended Testicles: A condition where one or both testicles failed to descend into the scrotum during fetal development.
A doctor will typically begin with a general physical examination and medical history. Key diagnostic tests include:
Semen Analysis: The primary test, which evaluates the volume, sperm concentration, motility (movement), and morphology (shape) of the sperm in a sample.
Hormone Testing: Blood tests to measure levels of testosterone and other key hormones that regulate sperm production.
Scrotal Ultrasound: Imaging to look for a varicocele or other structural problems in the testicles.
Genetic Tests: Blood tests to check for genetic abnormalities, especially in cases of extremely low sperm concentration.
Other tests: Including post-ejaculation urinalysis (to check for retrograde ejaculation) or a testicular biopsy.
Treatment depends on the underlying cause of infertility:
Surgery: Can be used to repair a varicocele (varicocelectomy), correct an obstructed sperm duct, or reverse a prior vasectomy.
Treating Infections: Antibiotics may clear a reproductive tract infection, but they do not always restore fertility.
Medication/Hormone Treatments: Recommended in cases where infertility is due to high or low levels of certain hormones.
Assisted Reproductive Technology (ART): These techniques are often used when other treatments are unsuccessful or if the cause cannot be corrected.
Sperm Retrieval: Procedures to surgically extract sperm directly from the testicles or epididymis if there is a blockage or no sperm in the ejaculate.
Intracytoplasmic Sperm Injection (ICSI): A single, healthy sperm is injected directly into an egg. This is a common and highly effective method, especially when sperm quality or quantity is poor.
In Vitro Fertilization (IVF): Sperm are combined with eggs in a lab dish for fertilization.
Intrauterine Insemination (IUI) / Artificial Insemination: A concentrated sample of sperm is inserted directly into the partner’s uterus.
Microdissection Testicular Sperm Extraction MicroTESE is a highly specialized microsurgical procedure used to retrieve sperm directly from the testicles of men who have no sperm in their ejaculate, a condition called azoospermia.
It is the preferred and most successful method for men diagnosed with Non-Obstructive Azoospermia ($\text{NOA}$), a condition where sperm production is severely impaired but may still be occurring in small, isolated areas of the testis. $\text{microTESE}$ allows for a meticulous search to locate these rare pockets of sperm production while minimizing damage to the surrounding testicular tissue.
The primary indication for this procedure is Non-Obstructive Azoospermia MicroTESE, which is typically due to a problem with sperm production rather than a blockage. You may be a candidate for MicroTES if:
You have azoospermia (no sperm in the ejaculate) confirmed by two separate semen analyses.
Your azoospermia is determined to be non-obstructive following a thorough clinical and hormonal evaluation.
You have high $\text{FSH}$ levels, small testicles, or abnormal genetics (e.g., Klinefelter syndrome, certain Y-chromosome microdeletions).
Prior, less invasive sperm retrieval attempts (such as conventional MicroTESE or MicroTESE have failed.
MicroTESE into a professional website page, using the provided MicroTESE document as a pattern.
Since you did not provide the text for Microdissection TESE, I will use the information I generated in the previous response to create the professional website page you requested.
Testicular Exposure: A single, small incision is made in the scrotum to access the testicle. The surgeon opens the tunica albuginea (the outer layer of the testicle).
Microsurgical Search: Using a high-magnification surgical microscope, the surgeon carefully examines the exposed seminiferous tubules across the entire testicle.
Targeted Extraction: The surgeon looks for dilated, opaque tubules, which are visually distinguished from the thin, translucent tubules that are typically associated with failure of sperm production. Only these promising tubules are selectively removed, minimizing the amount of tissue taken.
Immediate Lab Analysis: An experienced embryologist or technician immediately processes the minute tissue samples to locate and isolate viable sperm cells for use with MicroTESE or for MicroTESE .
Closure: The testicular membrane and the scrotal incision are closed with fine, dissolvable sutures.
Recovery: Most men recover quickly, with minimal discomfort managed by over-the-counter or prescribed pain medication. Patients are advised to avoid heavy lifting and strenuous activity for a period after the surgery.
Complications: Risks are low but can include swelling, bleeding, infection, and, rarely, a temporary or permanent decrease in testosterone production.
Result: A successful MicroTESE procedure provides the opportunity for men with even the most severe form of male infertility to become biological fathers using their own genetic material.
If you have been diagnosed with Non-Obstructive Azoospermia, consult with a specialist to determine if MicroTESE is the right pathway toward achieving your goal of biological fatherhood.
Sperm retrieval techniques are specialized medical procedures designed to obtain sperm directly from the male reproductive tract, particularly in men who have little or no sperm in their ejaculate (azoospermia). These advanced methods are used to enable conception through assisted reproductive technologies such as IVF (In-Vitro Fertilization) or ICSI (Intracytoplasmic Sperm Injection).
These procedures are performed by experienced urologists or andrologists under local or general anesthesia and are selected based on the underlying cause of infertility.
Sperm retrieval can be performed using various minimally invasive or surgical methods. The three commonly used procedures are TESA, PESA, and NAB.
TESA involves aspirating sperm directly from the testicular tissue using a fine needle. It is typically performed under local anesthesia and is ideal for men with non-obstructive azoospermia, where sperm production in the testis is low but still present.
Procedure Steps:
A fine needle is inserted into the testis.
A small sample of testicular tissue is aspirated.
The sample is processed in the laboratory to extract viable sperm.
Advantages:
Simple, minimally invasive, and quick.
Can often be performed on the same day as egg retrieval for the partner.
Limitations:
May yield limited sperm in some severe cases of testicular failure.
Repeat procedures may be required if no sperm are found.
PESA is used primarily for men with obstructive azoospermia, such as those with a vasectomy or congenital absence of the vas deferens. In this technique, sperm are collected from the epididymis — the coiled tube where sperm are stored after being produced in the testis.
Procedure Steps:
A fine needle is inserted into the epididymis through the scrotal skin.
Fluid containing sperm is aspirated.
The retrieved sperm are examined and processed for use in ICSI.
Advantages:
Quick and minimally invasive.
Often provides motile and mature sperm suitable for fertilization.
Limitations:
May need to be repeated if the sperm count in the aspirate is low.
Not suitable for men with non-obstructive azoospermia.
Needle Aspiration Biopsy is a simple and effective method to retrieve sperm directly from the testicular tissue using a small biopsy needle. It is often performed when TESA or PESA are unsuccessful or when a diagnostic tissue sample is also required.
Procedure Steps:
Under local anesthesia, a needle is inserted into the testis to remove a small tissue fragment.
The tissue is examined microscopically to locate and extract sperm.
Advantages:
Provides both diagnostic and therapeutic benefits.
Can be used for sperm retrieval and histological evaluation of testicular tissue.
Limitations:
May cause mild discomfort or swelling.
Requires skilled handling in the laboratory to isolate sperm.
Before performing sperm retrieval, a thorough evaluation is essential to identify the cause of azoospermia or low sperm count.
Diagnostic Assessments May Include:
Hormonal Evaluation: To assess testosterone, FSH, and LH levels.
Scrotal Ultrasound: To detect structural abnormalities or obstruction.
Genetic Testing: In cases of congenital or idiopathic infertility.
Physical Examination: To evaluate testicular size and consistency.
After sperm retrieval, mild discomfort, swelling, or bruising may occur, which usually resolves within a few days. Pain relief medications and scrotal support are often advised.
The retrieved sperm are either used immediately for ICSI or cryopreserved (frozen) for future use. The success rate depends on the underlying cause of infertility, sperm quality, and the chosen retrieval technique.
Sperm retrieval techniques are recommended in cases such as:
Absence of sperm in semen (azoospermia).
Obstruction of the vas deferens or epididymis.
Failure of vasectomy reversal.
Genetic or congenital absence of the vas deferens.
Ejaculatory dysfunction or retrograde ejaculation.
Sperm retrieval techniques (TESA, PESA, NAB) offer men with azoospermia a chance to father biological children through assisted reproductive technologies. Each method is chosen based on the patient’s condition, medical history, and cause of infertility.
Early evaluation by a qualified urologist or andrologist and timely intervention can greatly improve the chances of successful sperm retrieval and conception.
Vasectomy is a safe, simple, and highly effective surgical procedure for male sterilization or permanent contraception. It works by blocking or sealing the tubes that carry sperm (vas deferens), thereby preventing sperm from mixing with semen during ejaculation. The procedure does not affect sexual performance, testosterone levels, or the ability to achieve an erection or orgasm.
Vasectomy is chosen by men who have completed their family or wish to avoid future pregnancies through a reliable, permanent method.
Vasectomy can be performed using different techniques depending on the surgeon’s expertise and the patient’s preference. The two most common types are:
In this method, small incisions are made on both sides of the scrotum to access the vas deferens.
Procedure Steps:
The surgeon makes a tiny incision on the scrotum.
The vas deferens is cut and a small section may be removed.
The ends are then sealed by tying, cauterizing, or clipping.
The skin is closed with dissolvable stitches.
Advantages:
Well-established, safe, and effective technique.
Suitable for patients with complex anatomy.
Limitations:
Slightly longer recovery time compared to the no-scalpel method.
May cause minor discomfort or bruising post-surgery.
This is a minimally invasive technique that uses a small puncture instead of a surgical incision.
Procedure Steps:
A tiny puncture is made on the scrotal skin.
The vas deferens is gently pulled out, cut, and sealed.
No stitches are required as the puncture heals naturally.
Advantages:
Less bleeding, pain, and infection risk.
Faster recovery and minimal scarring.
Highly effective with success rates above 99%.
Limitations:
Requires specialized surgical training.
A small percentage of men may experience mild swelling or discomfort.
Before undergoing a vasectomy, your urologist will perform a detailed consultation and evaluation.
Pre-Procedure Steps Include:
Medical history review and physical examination.
Discussion about permanence and alternatives.
Stopping certain medications (like blood thinners) if advised.
Shaving and cleaning the scrotal area before surgery.
Recovery after vasectomy is typically quick and uncomplicated. Most men can return to normal activities within 2–3 days.
Post-Operative Instructions:
Apply ice packs to reduce swelling.
Wear supportive underwear for comfort.
Avoid heavy lifting or strenuous activity for one week.
Keep the area clean and dry.
Use pain relief medication as prescribed.
It’s important to note that sterility is not immediate. Sperm may still be present in the semen for several weeks. A follow-up semen analysis after about 8–12 weeks is necessary to confirm a zero sperm count before discontinuing other contraceptive methods.
Permanent and highly reliable contraception (over 99% effective).
No ongoing cost or need for repeated procedures.
Does not affect sexual desire, erection, or ejaculation.
Minimally invasive with quick recovery.
Safer and simpler than female sterilization.
hough vasectomy is generally safe, some men may experience mild side effects, including:
Temporary pain or swelling.
Minor bleeding or bruising at the incision site.
Formation of small lumps (sperm granulomas).
Rarely, infection or chronic scrotal discomfort.
Most of these issues are short-term and resolve with conservative management.
While vasectomy is designed to be permanent, vasectomy reversal (vasovasostomy) is sometimes possible. However, the success rate of reversal depends on how much time has passed since the original surgery and individual health factors.
Vasectomy is a safe, simple, and permanent solution for male contraception. It offers an effective and convenient method of birth control for men who have completed their family planning. The procedure is quick, minimally invasive, and has minimal impact on sexual function or hormone levels.
Consult an experienced urologist or andrologist to understand the benefits, procedure details, and post-surgical expectations before making an informed decision.
Vasectomy Reversal is a microsurgical procedure designed to restore fertility in men who have previously undergone a vasectomy. The surgery reconnects the vas deferens, the tubes that were cut or sealed during vasectomy, allowing sperm to once again be present in the semen.
Many men choose vasectomy reversal when they wish to father a child after a change in personal circumstances, such as remarriage, loss of a child, or a change in family plans.
This procedure is delicate and requires the expertise of an experienced urologist or microsurgeon specializing in male fertility.
There are two main types of vasectomy reversal surgeries. The choice depends on the patient’s anatomy and findings during the operation.
Vasovasostomy is the most common type of reversal surgery. It involves directly reconnecting the two cut ends of the vas deferens to restore the passage for sperm.
Procedure Steps:
Performed under general or regional anesthesia.
A small incision is made in the scrotum to expose the vas deferens.
The surgeon examines the fluid from the vas end closest to the testis.
If sperm are present, the two ends of the vas deferens are carefully reconnected using microscopic sutures.
Advantages:
High success rates when sperm are found in the vasal fluid.
Allows natural conception in many cases.
Limitations:
Success depends on the time elapsed since the vasectomy.
Requires precise microsurgical skills.
This procedure is performed when there is a blockage between the vas deferens and the epididymis, and sperm are not found in the vasal fluid during surgery.
Procedure Steps:
The surgeon connects the vas deferens directly to the epididymis.
This bypasses the blockage and allows sperm to mix with semen again.
Advantages:
Effective in cases of long-standing vasectomy or epididymal blockage.
Restores the pathway for sperm when vasovasostomy is not possible.
Limitations:
Technically more complex and time-consuming.
Success rates are slightly lower than vasovasostomy.
Before the surgery, a detailed evaluation helps determine the best surgical approach and predict the chances of success.
Assessment May Include:
Medical History Review: To understand any prior surgeries or health issues.
Physical Examination: To assess the condition of the scrotum and vas deferens.
Partner Evaluation: Female partner’s age and fertility status are also considered.
Blood Tests or Imaging: Sometimes used to check hormone levels or detect obstruction.
Recovery after vasectomy reversal is generally smooth, but careful postoperative management helps achieve the best results.
Post-Surgery Guidelines:
Mild discomfort, swelling, or bruising may occur for a few days.
Apply cold packs to reduce swelling.
Avoid strenuous activities or sexual intercourse for 2–3 weeks.
Pain relief and antibiotics may be prescribed.
Wear supportive undergarments for comfort.
Follow-up semen analyses are performed every few weeks to check for the presence of sperm in the semen. It may take 3 to 6 months for sperm to reappear, depending on the individual healing process.
Vasectomy Reversal offers men a renewed opportunity for natural conception after vasectomy. With advanced microsurgical techniques like Vasovasostomy and Vasoepididymostomy, success rates are high and outcomes are favorable when performed by a skilled urologist.
If you are considering fathering a child after a vasectomy, consult an experienced urologist or andrologist to determine the best surgical option and improve your chances of restoring fertility.
Penile Vibratory Stimulation (PVS) is a non-invasive medical procedure used to induce ejaculation in men with spinal cord injury, ejaculatory dysfunction, or neurological conditions that prevent normal ejaculation. This technique uses a specialized medical vibrator to stimulate the nerves at the tip of the penis, triggering a natural ejaculatory reflex.
It is a safe, effective, and painless method widely used in assisted reproductive techniques to collect semen for fertility evaluation or assisted conception.
PVS is primarily used for:
Men with spinal cord injuries above the T10 level.
Men who are unable to ejaculate due to neurological disorders.
Semen collection for assisted reproduction such as IUI, IVF, or ICSI.
Fertility evaluation when natural ejaculation is not possible.
Diagnostic testing of ejaculatory and autonomic nerve function.
The procedure relies on high-frequency vibration applied to the glans penis (head of the penis), which activates the ejaculatory reflex through the pudendal and pelvic nerves. This results in rhythmic contractions of the seminal vesicles, prostate, and vas deferens — producing ejaculation.
Preparation:
The patient is positioned comfortably, usually lying down.
The genital area is cleaned to maintain hygiene.
In some cases, mild sedation or relaxation techniques may be used.
Stimulation:
A medical-grade vibrator is applied to the glans penis.
Vibration is maintained for short intervals until ejaculation occurs.
The procedure usually takes 5 to 10 minutes.
Semen Collection:
Ejaculated semen is collected in a sterile container.
If ejaculation occurs retrogradely (into the bladder), urine may be collected and processed to retrieve sperm.
Post-Procedure:
The sample is analyzed for sperm count, motility, and morphology.
If adequate, it can be used immediately for assisted reproductive techniques such as IUI or IVF-ICSI.
PVS is indicated in the following conditions:
Spinal Cord Injury (SCI): Especially in men with lesions above T10.
Multiple Sclerosis and other neurodegenerative diseases.
Diabetic Neuropathy causing ejaculatory dysfunction.
Retrograde Ejaculation when partial emission occurs.
Unexplained Ejaculatory Failure where other methods are not effective.
Non-invasive: No surgery or anesthesia required.
Safe and Painless: Well-tolerated by most patients.
Quick Procedure: Usually completed within 10–15 minutes.
Effective: High success rates in men with upper spinal cord injuries.
Useful for Assisted Reproduction: Provides viable sperm for IUI or IVF without invasive retrieval.
May not work effectively in men with lower spinal cord injuries (below T10).
Some patients may require additional procedures such as Electroejaculation (EEJ) if ejaculation is not achieved.
The semen quality may vary depending on the underlying condition.
Not suitable for men with severe penile sensitivity loss or peripheral nerve damage.
PVS is extremely safe when performed under medical supervision. Rare side effects include:
Mild penile redness or discomfort due to vibration.
Transient changes in heart rate or blood pressure (in spinal cord injury patients).
Rarely, autonomic dysreflexia in men with high spinal cord injuries — managed by monitoring during the procedure.
PVS should be considered when:
A man with spinal cord injury or neurological dysfunction wishes to have biological children.
Natural ejaculation is not possible despite normal sperm production.
Non-invasive sperm retrieval is preferred before surgical options like TESA or PESA.
Semen samples are needed for assisted reproductive techniques.
Penile Vibratory Stimulation (PVS) is a safe, simple, and effective technique for inducing ejaculation in men with spinal cord injuries or ejaculatory disorders. It plays an important role in fertility preservation and assisted reproduction by allowing semen collection without invasive procedures.
Under the supervision of a skilled urologist or andrologist, PVS offers men with ejaculatory dysfunction a reliable path to biological parenthood.
Transurethral Resection of Ejaculatory Ducts (TURED) is a minimally invasive surgical procedure used to treat ejaculatory duct obstruction (EDO) — a condition where the ducts that carry semen from the seminal vesicles and vas deferens into the urethra become blocked.
This obstruction can lead to infertility, low semen volume, painful ejaculation, or absence of sperm (azoospermia) despite normal sperm production in the testes.
TURED aims to remove the blockage, restore normal semen flow, and improve fertility outcomes.
The ejaculatory ducts are small channels that open into the prostatic urethra and allow the passage of semen during ejaculation. When these ducts are blocked (due to cysts, inflammation, or congenital abnormalities), sperm cannot exit the body.
TURED is performed to:
Relieve ejaculatory duct obstruction.
Restore normal semen volume and flow.
Improve fertility potential.
Relieve painful ejaculation or pelvic discomfort.
TURED is recommended in men who present with:
Low-volume azoospermia or oligozoospermia (very little or no sperm in semen).
Painful ejaculation or pelvic pain.
Recurrent prostatitis-like symptoms.
Dilated seminal vesicles or ejaculatory duct cysts on imaging.
Infertility with confirmed obstruction on diagnostic tests.
Before performing TURED, a detailed evaluation is necessary to confirm the diagnosis of ejaculatory duct obstruction and rule out other causes of infertility.
Diagnostic Tests May Include:
Semen Analysis: Shows low semen volume, acidic pH, and absent or few sperm.
Transrectal Ultrasound (TRUS): Detects cysts, calcifications, or dilated seminal vesicles.
MRI Pelvis: Provides detailed visualization of the ejaculatory ducts and surrounding structures.
Vasography or Seminal Vesiculography: Sometimes used to map the site of obstruction.
Hormonal Profile: To rule out testicular or endocrine causes of azoospermia.
Anesthesia:
The procedure is performed under spinal or general anesthesia for comfort.
Endoscopic Access:
A resectoscope (a thin, lighted instrument) is inserted through the urethra up to the prostatic urethra.
Identification of Ejaculatory Ducts:
The surgeon identifies the verumontanum — the area where the ejaculatory ducts open.
Resection of the Obstruction:
A small section of tissue overlying the ejaculatory ducts is removed (resected) to open the blocked channels.
Any cysts, stones, or obstructions are cleared to restore semen flow.
Flushing and Inspection:
The seminal vesicles may be flushed with saline to ensure patency.
The procedure is completed within 30–45 minutes.
Recovery:
A urinary catheter may be placed temporarily and removed after 24 hours.
After TURED, recovery is usually quick, and most patients can return to normal activities within a few days.
Post-Surgery Guidelines:
Mild burning or blood in urine for a few days is normal.
Drink plenty of fluids to keep the urinary tract clear.
Avoid sexual activity or heavy exertion for 2–3 weeks.
Use prescribed antibiotics and pain relief as directed.
A follow-up semen analysis is done after 6–8 weeks to assess improvement in sperm output.
Restores natural semen flow and ejaculation.
Improves sperm count and fertility potential.
Relieves pelvic or ejaculatory pain.
Minimally invasive with quick recovery.
Avoids the need for more complex fertility procedures in suitable cases.
Transurethral Resection of Ejaculatory Ducts (TURED) is a highly effective and minimally invasive procedure for treating ejaculatory duct obstruction, a reversible cause of male infertility.
By restoring the normal passage of semen, TURED can significantly improve ejaculatory function, sperm count, and chances of natural conception.
Consult an experienced urologist or andrologist to determine if TURED is the appropriate treatment option based on your diagnostic evaluation and fertility goals.
Dr. Rohit Kaushal is a leading Urologist and Robotic Surgeon in Delhi, specializing in kidney transplant, prostate, and reconstructive urology with compassionate patient care.
© 2025 Created with Digital Growth Well